The Biodefense Graduate Program will be hosting the Pandemics and Global Health Security Workshop in July! Danyale Kellogg, an incoming student to the Biodefense PhD program, highlights the security concerns related to the ending of smallpox vaccinations. Several states are devising incentives to increase their rates of COVID-10 vaccinations.
Event – Pandemics and Global Health Security Workshop
COVID-19 has exposed just how unprepared governments, corporations, and societies are for a global pandemic. While the SARS-CoV-2 virus is only the most recent threat to global health security, it will certainly not be the last. Threats to global health security continue to evolve due to the emergence of new infectious diseases, globalization, advances in science and technology, and the changing nature of conflict. Pandemics and Global Health Security is a three-day virtual, non-credit workshop designed to introduce participants to the challenges facing the world at the intersection of pandemic preparedness and response, public health, national security, and the life sciences. Over the course of three days, participants will discuss how the biology and epidemiology of SARS-CoV-2 contributed to the emergence of that virus as a global pandemic, lessons learned from Operation Warp Speed about the development of medical countermeasures, obstacles to hospital biopreparedness, challenges to science communication during a pandemic, the bioethics of resource allocation during a public health emergency, the future of global health security, and the role of science and technology in preventing and responding to pandemics. The workshop faculty are internationally recognized experts from the government, private sector, and academia who have been extensively involved in research and policy-making on public health, biodefense, and security issues. Live, interactive sessions will include Dr. Rick Bright, The Rockefeller Foundation; Dr. Nicholas G. Evans, University of Massachusetts-Lowell; Dr. Andrew Kilianski, Department of Defense; Dr. Gregory D. Koblentz, George Mason University; Dr. Jennifer Nuzzo, Johns Hopkins Center for Health Security; Dr. Saskia Popescu, George Mason University; Dr. Angela L. Rasmussen, Vaccine and Infectious Disease Organization-International Vaccine Centre; and Jessica Malaty Rivera, COVID Tracking Project. The workshop is organized by the Biodefense Graduate Program at the Schar School of Policy and Government at George Mason University and will be held virtually on July 19-21, 2021. Each day will run from 9am to 12:30pm ET. Register here.
Toward A Whole-of-Society Framework for Countering Disinformation
Disinformation is the deliberate dissemination of false or erroneous information in order to discredit a person, organization, product, or notion. Disinformation is used as a tactic by actors ranging from Russia’s campaign to weaken democratic and international institutions to terrorist groups’ recruitment efforts to the growing anti-vaccine movement. JD Maddox, Casi Gentzel, and Adela Levis describe a framework for countering disinformation that would entail not only “counter messaging but also of proactive measures that use facts to inform audiences, reduce the impact of disinformation, and promote freedom of expression.” The framework categorizes efforts as communication, resilience, disruption, or regulation. Proactive communication before disinformation (or misinformation) can gain a foothold is critical and requires “implementation of the full spectrum of communication capabilities.” Further, increasing transparency and building trust in democratic values and institutions are needed. Building resilience to disinformation will include activities such as improving digital literacy; promoting independent, fact-based, investigative journalism; and leveraging public diplomacy. Disruption leverages technology to prevent the spread of disinformation through various tools and techniques such as blocking or cyberspace operations. Regulation – including legislation and international cooperation – should seek input from local and national legislators, media associations, internet platforms and the broader tech sector, and international organizations. JD Maddox will be teaching a course for the Schar School next semester on countering disinformation. Read the article here.
The Overlooked, Dangerous Nexus Between National Security and Public Health: The Case of Smallpox
Danyale Kellogg, an incoming student to the Biodefense PhD program, highlights the security concerns related to the ending of smallpox vaccinations for the civilian population after the disease’s eradication in 1980. Today, only the US and Russia maintain official samples of the variola virus that causes smallpox; however, other nations possess unofficial samples of the virus, including North Korea. This sparks concerns that a country possessing samples could deploy them as a weapon, an attack that the US is ill-equipped to combat. Additionally, there are worries regarding the use of artificial gene synthesis to recreate smallpox. In fact, in 2017, a Canadian research team synthesized the horsepox virus, which as a relative to smallpox could serve as a roadmap to recreating the eradicated scourge. Preparing for a possible smallpox attack would require “strengthening public health at all levels, ensuring the stability and efficacy of the Strategic National Stockpile, and making sure healthcare providers and private healthcare systems are prepared should they be presented with a case.”
Top Researchers are Calling for a Real Investigation into the Origin of COVID-19
Eighteen prominent biologists published a letter in the journal Science calling for a new investigation into all conceivable origins of the novel coronavirus, and imploring that Chinese laboratories and agencies “open their records” to independent analysis. They write:
“As scientists with relevant expertise, we agree with the WHO director-general, the United States and 13 other countries, and the European Union that greater clarity about the origins of this pandemic is necessary and feasible to achieve. We must take hypotheses about both natural and laboratory spillovers seriously until we have sufficient data. A proper investigation should be transparent, objective, data-driven, inclusive of broad expertise, subject to independent oversight, and responsibly managed to minimize the impact of conflicts of interest. Public health agencies and research laboratories alike need to open their records to the public. Investigators should document the veracity and provenance of data from which analyses are conducted and conclusions drawn, so that analyses are reproducible by independent experts.”
The controversial theory that the virus could have escaped from the Wuhan Institute of Virology (WIV) remains a point of contention, but the letter calls for a thorough examination of all possibilities. Dr. Shi Zhengli, chief scientist for emerging disease at WIV, said that the “letter’s suspicions were misplaced and would damage the world’s ability to respond to pandemics.”
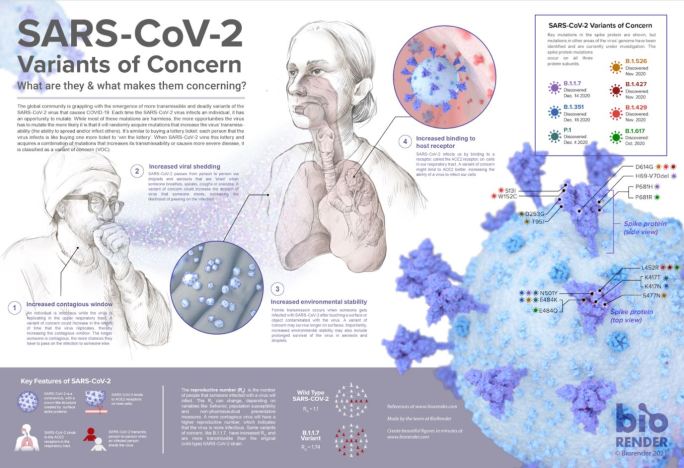
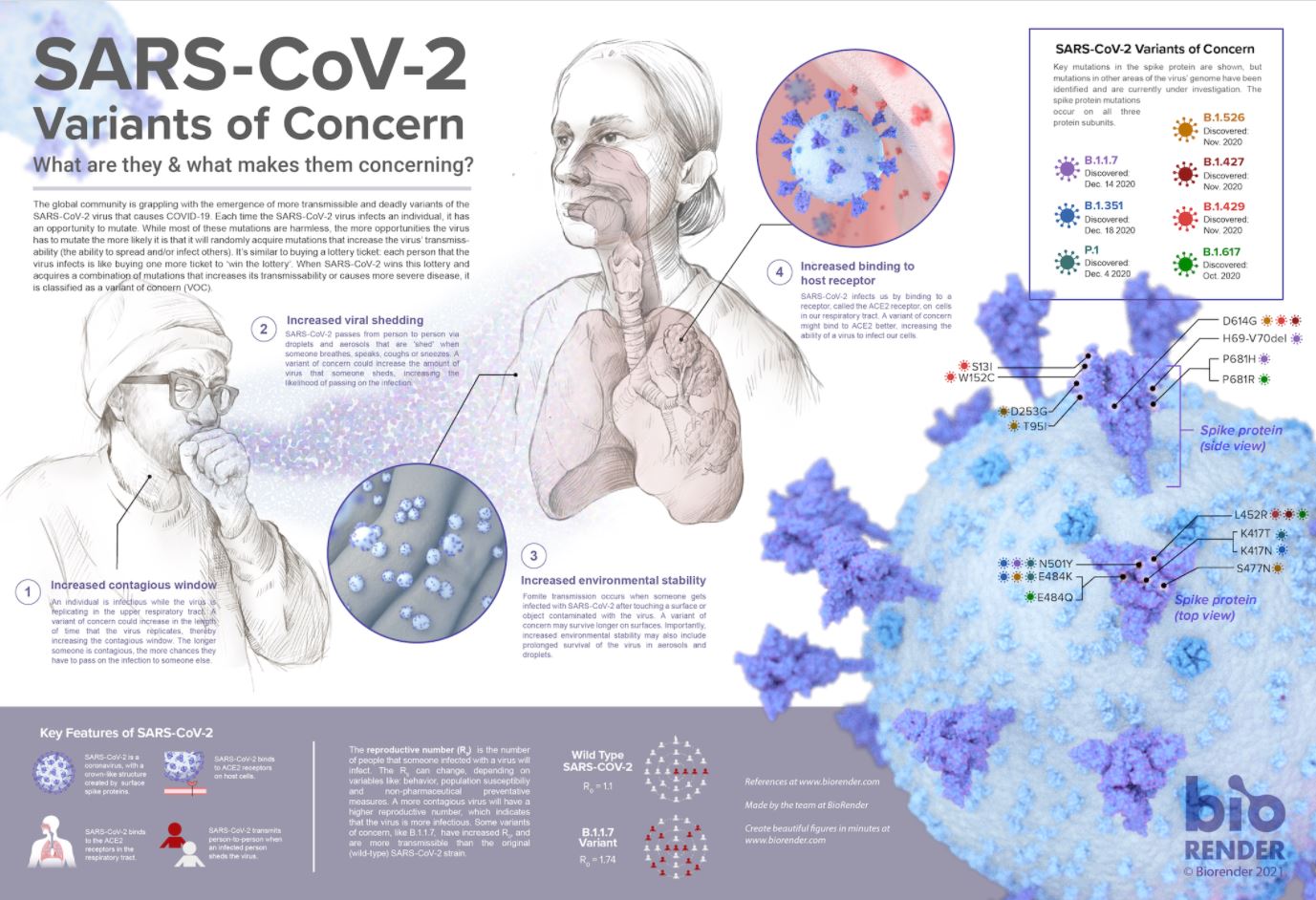
Infographic on SARS-CoV-2 Variants of Concern with Dr. Angela Rasmussen
Dr. Angela Rasmussen, a virologist and research scientist with the Georgetown Center for Global Health Science and Security and VIDO-InterVac at the University of Saskatchewan, developed an infographic explaining the most important features of the newest SARS-CoV-2 variants.
NTI and the Next Generation GHS Network Launch 5th Annual Next Generation for Biosecurity Competition
NTI | bio is partnering with the Next Generation Global Health Security (GHS) Network to launch the fifth annual Next Generation for Biosecurity Competition to foster biosecurity professional development within the Next Generation GHS Network. We are seeking innovative and creative papers for online publication by NTI | bio and the NextGen GHS Network focused on responsible conduct of life science research. The winning team also will receive travel and lodging support to attend and present during a side-event at the 2021 Biological Weapons Convention Meeting of States Parties in Geneva.
As emerging biological risks continue to grow with the rapid pace of biotechnology advances, safe, secure, and responsible conduct of life science research is increasingly important. For this year’s competition, submissions should address the following questions and subordinate considerations: What life science research should not be conducted, if any? Should red lines in life science research be drawn? If so, by whom?
Information regarding submission criteria and eligibility can be found here. The deadline is 28 June 2021 at 11:59 PM EST.
Expert Independent Panel Calls for Urgent Reform of Pandemic Prevention and Response Systems
A panel of leading experts is calling on the global community to end the COVID-19 pandemic by immediately implementing a series of bold recommendations to redistribute, fund, and increase the availability of and manufacturing capacity for vaccines, and to apply proven public health measures urgently and consistently in every country. The Panel is also recommending that national governments and the international community immediately adopt a package of reforms to transform the global pandemic preparedness and response system and prevent a future pandemic. The Independent Panel for Pandemic Preparedness and Response was appointed by the World Health Organization (WHO) Director-General in response to a World Health Assembly resolution calling for an independent, impartial, and comprehensive review of experiences gained and lessons to be learned from the current pandemic. The review was also asked to provide recommendations to improve capacity for global pandemic prevention, preparedness, and response. The Panel released its findings and recommendations today in its main report: COVID-19: Make it the Last Pandemic. The report demonstrates that the current system—at both national and international levels— was not adequate to protect people from COVID-19. The time it took from the reporting of a cluster of cases of pneumonia of unknown origin in mid-late December 2019 to a Public Health Emergency of International Concern being declared was too long. February 2020 was also a lost month when many more countries could have taken steps to contain the spread of SARS-CoV-2 and forestall the global health, social, and economic catastrophe that continues its grip. The Panel finds that the system as it stands now is clearly unfit to prevent another novel and highly infectious pathogen, which could emerge at any time, from developing into a pandemic. Recommended reforms include: establishing a Global Health Threats Council; establishing a new global system for surveillance based on full transparency; investing in national preparedness now; and creating an International Pandemic Financing Facility.
Poll Finds Public Health Has A Trust Problem
A poll conducted by the Robert Wood Johnson Foundation and the Harvard T.H. Chan School of Public Health surveyed 1,305 people from mid-February to mid-March of this year to examine trust in key public health groups. The survey found that merely 52% of respondents have a great deal of trust in the Centers for Disease Control and Prevention (CDC), but other agencies saw even lower figures. Only 37% said they had a lot of trust in the National Institutes of Health (NIH) or the Food and Drug Administration (FDA). Forty-one percent trust state health departments and 44% trust local health departments. This growing mistrust is unsurprising given the many missteps that have occurred in the COVID-19 pandemic including political interference, incomplete information, and confusing messaging. Interestingly, the survey showed the political divide in trust: only 27% of Republicans greatly trust the CDC, compared to 76% of Democrats.
Modeling of Future COVID-19 Cases, Hospitalizations, and Deaths, by Vaccination Rates and Nonpharmaceutical Intervention Scenarios
A recent Morbidity and Mortality Weekly Report (MMWR) from the Centers for Disease Control and Prevention (CDC) modelled the expected COVID-19 cases, hospitalizations, and deaths. Increases in COVID-19 cases in March and early April occurred despite a large-scale vaccination program. Increases coincided with the spread of SARS-CoV-2 variants and relaxation of nonpharmaceutical interventions (NPIs). Data from six models indicate that with high vaccination coverage and moderate NPI adherence, hospitalizations and deaths will likely remain low nationally, with a sharp decline in cases projected by July 2021. Lower NPI adherence could lead to substantial increases in severe COVID-19 outcomes, even with improved vaccination coverage. High vaccination coverage and compliance with NPIs are essential to control COVID-19 and prevent surges in hospitalizations and deaths in the coming months.
What Has COVID-19 Taught Us about Strengthening the DOD’s Global Health Security Capacities?
A new report from the Center for Strategic and International Studies (CSIS) details five recommendations for “how the Biden-Harris administration and members of Congress can help steer impending deliberations over the future of the DOD’s contributions to global health security.” The COVID-19 pandemic has cost millions of lives and sickened many more, destabilizing economies and security. Though we are not yet out of the woods with this pandemic, we should prepare to face biological threats in the future. Broad US military expertise in health, biosecurity, and biosafety has contributed to the ongoing response and will continue to contribute substantially to coordinated, interagency global health security efforts. These recommendations are designed to “complement the excellent and extensive recent analysis by Mark Cancian and Adam Saxton of the CSIS International Security Program on how the US military responded to Covid-19 to guarantee the protection and readiness of US forces and how it supported the civilian pandemic response at home.” The recommendations are: (1) elevate biological threats; (2) protect and strengthen operational assets; (3) secure the future of the DOD’s medical skill base; (4) launch a military-to-military health security cooperation initiative; and (5) transition existing DOD international health engagement activities into sustainable, integrated programs. Read the report here.
Upcoming Meeting of the National Biodefense Science Board
The National Biodefense Science Board (NBSB) provides expert advice and guidance to the Secretary of the US Department of Health and Human Services and the Assistant Secretary of Preparedness and Response on scientific, technical, and other matters related to public health emergency preparedness and response. The NBSB will host a public teleconference to discuss new recommendations to HHS that address remaining public health emergency preparedness and response challenges. In light of the numerous health emergencies and disasters that have affected the United States since 2007, NBSB continues to provide recommendations related to health emergency preparedness, response, and recovery. Meetings of the NBSB are open to the public. This meeting will be held on 26 May 2021 at 11 AM EST. Register here.
Event – Get Set: Lessons Learned for The Biological and Toxin Weapons Convention Review Conference
The United Nations Institute for Disarmament Research (UNIDIR) is hosting an online discussion on Lessons Learned for the Biological and Toxin Weapons Convention (BWC) Review Conference. This is the second in a series of events the Institute is hosting in preparation for the Review Conference of the Biological and Toxin Weapons Convention. The event will contribute to enhancing understandings of BWC review conferences and identifying lessons to be learned from past experiences. Speakers for this event include Ambassador Dr. György Molnár, Special Representative of the Minister of Foreign Affairs and Trade for Arms Control, Disarmament and Non-Proliferation MFAT Hungary and President of the Eighth BWC Review Conference; Dr. Una Jakob, research associate at the Peace Research Institute Frankfurt (PRIF) in Germany; and Mr. Zahid Rastam, charge d’Affaires ad-interim, High Commissioner of Malaysia to United Kingdom. The panel will be moderated by UNIDIR researcher, James Revill and will include a question-and-answer session with the audience. The event will be held 20 May 2021 at 1 PM CEST. Register here.
Ineffective Past, Uncertain Future
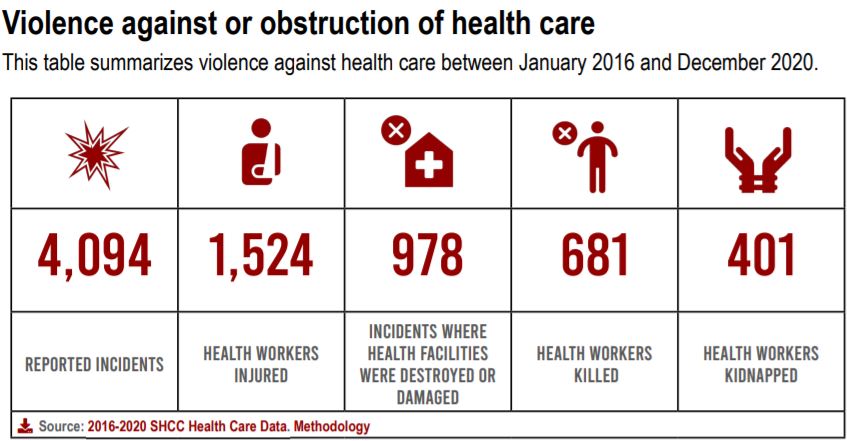
In 2016, in the face of relentless attacks on health care in situations of conflict, the UN Security Council adopted Resolution 2286. This committed UN member states to taking action to prevent attacks on health care and ensure accountability for perpetrators. In the five years since, they have done neither. In annual reports in the years since Resolution 2286 was adopted, the Safeguarding Health in Conflict Coalition (SHCC) and Insecurity Insight reported a total of more than 4,000 unique incidents of violence against health care in situations of armed conflict – on average more than two incidents a day. Because the reporting of such incidents is limited in many countries, this number is likely a significant undercount. The violence has taken myriad forms: airstrikes against and shelling of hospitals and clinics; kidnappings and killings of health workers; damage to, the destruction of, and looting of health care facilities and vehicles; actions that prevent those in need from accessing health care; violent interference with emergency medical responders, vaccinators and others and; arrests of health workers. During 2020, the COVID-19 pandemic resulted in more violence against health care, including in countries not at war, such as India and Mexico. Violence causes not only immediate death, injury, and destruction, but often results in an enormous psychological and physical toll on health workers and the people in the communities they serve. Hidden in each incident is the loss of family members and colleagues, livelihoods, homes, and, sometimes, a way of life. The true cost of the attacks also includes the lasting impacts on health workers’ mental health and on communities’ ability to access care for chronic illness, safe childbirth, immunization, and more. Fewer health workers are available to provide care as doctors and nurses flee the violence. The report – Ineffective Past, Uncertain Future – presents the documented threats and violence against health care between January 2016 and December 2020. An interactive map developed by Insecurity Insight and MapAction for the Safeguarding Health in Conflict Coalition shows incidents of violence and threats against health care. Read the report here and view the map here.
Incentives to Vaccinate
In effort to encourage COVID-19 vaccination, several states have devised clever incentivizes to increases their rates as demand declines. In Louisiana, the vaccine is easily accessible, but to inspire more people to join the fight against the pandemic, a vaccination event in New Orleans also offered a pound of free boiled crawfish. In Ohio, there will be five weekly lottery drawings for $1 million open to residents who received at least one dose of a COVID-19 vaccine. Similarly, there is a lottery for teenagers that offers a full, four-year scholarship to a public university in Ohio – room and board included. Maryland launched an incentive of $100 to state employees who opt to get fully vaccinated. New Jersey introduced its “Operation Jersey Summer” campaign to reach the state’s goal of vaccinating 70% of the adult population by the end of June. As part of the campaign, vaccinees aged 21 years or older can participate in the “Shot and a Beer” program that provides a free beer with COVID-19 vaccinations beginning this month.