For Biodefense graduate students looking for a fascinating course to round out your spring semester, Dr. Robert House is offering a course on the development of vaccines and therapeutics, and Dr. Quattrochi is teaching a course on biotechnology and society! The Bioeconomy Information Sharing and Analysis Center, or BIO-ISAC, released an advisory regarding an advanced persistent threat (APT) attack named Tardigrade. The World Health Assembly agreed to kickstart a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.
Spring 2022 Open Courses: BIOD 762 & 766
For any GMU graduate students, the Biodefense Program is offering a couple fascinating courses this coming spring semester! Biotechnology and Society (BIOD 762) examines the growing role of biotechnology in modern society, including benefits to human and animal health, industrial applications, and potential for misuse. This course will be taught by Dr. Lauren Quattrochi, a classically trained as an electrophysiologist and neuro-pharmacologist. Development of Vaccines and Therapeutics (BIOD 766) is possibly more relevant now than ever before! The course analyzes the process of developing new medical countermeasures against biological weapons and emerging infectious diseases such as SARS and pandemic influenza, and gives special attention to the scientific, technical, political, regulatory, and economic obstacles to developing new vaccines and therapeutics. Dr. Robert House, who has a PhD in medical parasitology and is Senior Vice President of Government Contracts at Ology Bioservices, will be teaching BIOD 766.
Agricultural Production, Traditional Foods and Household Food Insecurity in Rural Kenya: Practice, Perception and Predictors
Although rural households in Kenya rely on agricultural production for their livelihood, attaining food security is challenging in areas experiencing harsh agro-ecological conditions. We utilized mixed methods research to examine the effect of agricultural production, including that of traditional foods, on household food insecurity in Seme sub-County of Kenya. Study participants believed that traditional foods protected against hunger. However, production of these foods, with the exception of traditional vegetables, was low. Poultry-keeping; cereal/grain, any vegetable and traditional vegetable production; and crop diversity were significantly associated with lower household food insecurity. Vegetable production maintained statistical significance after controlling for other variables. Professor Bonnie Stabile, Associate Professor and Associate Dean of Student and Academic Affairs in the Schar School, was a co-author of this publication. Phil Thomas is an adjunct professor for the Biodefense Graduate Program who teaches the Threats to Global Food Security course. Read the article here.
You Should Be Afraid of the Next ‘Lab Leak’
In Boston stands a seven-story fortress that houses the National Emerging Infectious Diseases Laboratories (NEIDL), and it contains a large collection of Biosafety Level 4 and Biosafety Level 3 labs. These high-containment labs conduct research on some of the deadliest pathogens, like Lassa and Marburg viruses. An accident that resulted in one of these lethal microbes escaping could spur another outbreak and even another pandemic. Six years ago, the National Institutes for Health commission Gryphon Scientific, a consulting firm, to conduct a risk assessment of certain types of research at US facilities. The assessment led to a thousand-page report, which found that “that experiments to improve the transmissibility of coronaviruses in a lab could significantly increase the chance of a pandemic due to a laboratory accident.” It also noted that “loss of containment” incidents for viruses are rare, and that a breach would “not necessarily mean an outbreak.” Even an escaped pathogen with pandemic potential “would have a low chance of leading to a global crisis.”
Dr. Filippa Lentzos and Dr. Gregory Koblentz conducted a study of Biosafety Level 4 labs around the world and calculated that there are 59 in operation, under construction, or in the planning stages. Lentzos stated that “these labs are there so we can work with these pathogens in safe, secure ways,” but “these labs are spreading into other parts of the world, where you have different kinds of regimes, more authoritarian regimes, for instance, where the concept of openness is particularly challenging.”
Public & Private Funding Opportunities to Advance a Circular US Bioeconomy and Maintain US Biotechnology Competitiveness
In the nearly 50 years since the first genetic engineering experiments, the United States has become the world’s biotechnology powerhouse, with the resulting biology-based economy—the bioeconomy—generating nearly $960 billion in economic activity in 2016, about 5 percent of US GDP, with more than half of the total generated outside the biomedical sector, including the agricultural and industrial biotechnology sectors. Over the next two decades or less, a well-developed bioeconomy has the potential to transform manufacturing processes to use renewable biomass rather than petroleum to make the products of modern society, and in doing so, reduce the nation’s dependence on fossil fuels, revitalize US manufacturing and employment across the nation, create a more resilient supply chain, improve the nation’s health, and contribute significantly to the goal of creating a net zero greenhouse gas economy. However, decentralized leadership, inadequate talent development, insufficient investment in both fundamental research and developing bioprocessing infrastructure, and international competition put the United States at risk of forfeiting that world-leading position and squandering the entrepreneurial drive and capital market interest that is trying to expand the bioeconomy. Without concrete action to address these concerns, the nation’s economy, its national security, the health of its residents, and its opportunity to move to a net zero economy that creates good-paying jobs and keeps them in the country are in peril.
Schmidt Futures, a philanthropic initiative of Eric and Wendy Schmidt, convened a Task Force to chart a course for achieving the promise of platform technologies such as synthetic biology and artificial intelligence to contribute to what has recently been projected to become a future $4 trillion global bioeconomy. The Task Force deliberated the roadblocks and focused on identifying opportunities for translating basic science research into products for the general public by enabling large scale production of exciting bioeconomy products that are ready to move out of the lab, such as:
- a new generation of plastics that degrade to harmless chemicals in seawater and soil
- biologically produced, carbon-neutral cement
- alternative food protein sources that use less water and land and produce fewer greenhouse gas emissions
- climate change resilient plants, including salt- and drought-resistant crops
- textiles and dyes whose production slashes carbon dioxide emissions and reduces toxic waste
- soil microbes that reduce fertilizer use, improve the health of soils, and remove carbon dioxide from the atmosphere
This report from makes recommendations for public and private action that fall into two broad categories: foundational science and technology challenges and scale-up capacity bioproduction infrastructure. Read the report here.
Results of a 2020 Survey on Reporting Requirements and Practices for Biocontainment Laboratory Accidents
Biosafety laboratory accidents are a normal part of laboratory science, but the frequency of such accidents is unclear due to current reporting standards and processes. To better understand accident reporting, a survey was created, with input from ABSA International, which included a series of questions about standards, requirements, and likely motivations for reporting or nonreporting. A total of 60 biosafety officers completed the survey. Respondents reported working with more than 5,000 people in laboratories, including more than 40 biosafety level 3 or animal biosafety level 3 laboratories, which work with higher-risk pathogens. Most of the respondents were located in the United States, Canada, or New Zealand, or did not identify their location. Notable results included that 97% of surveyed biosafety officers oversee laboratories that require reporting exposure to at least some pathogens. However, 63% relayed that the reports are not usually sent outside of the institution where they occurred. A slight majority (55%) stated that paper reports were used, with the rest reporting they used a variety of computer systems. Even in laboratories that used paper-based reporting systems, 67% relayed that these reports were used alongside, or entered into, a digital system. While 82% of these biosafety officers agreed that workers understood the importance of reporting for their own safety, 82% also agreed that a variety of disincentives prevent laboratory workers from reporting incidents, including concerns about job loss and loss of funding. Read the article here.
As Supply Lines Strain, Some Corporations Rewrite Production Playbook
The COVID-19 pandemic interrupted a number of supply chains across the globe. Now, 23 months in, companies are still struggling to strengthen their supply chains. For example, Stanley Black & Decker has accelerated plans to open two new factories, one in Mexico and one in Texas. The company has also “locked in future supplies of lithium-ion batteries for power tools by funding dedicated production capacity at US and Taiwanese suppliers and stockpiled an extra $1 billion in products.” Don Allan, the chief financial officer of Stanley Black & Decker, said, “the more you can minimize the amount of time your product is in transit, the better off you’re going to be.” Companies are employing an array of tactics to solve their supply chain problems, at least temporarily. Colgate Palmolive used more expensive airfreight to ship its toothpaste and toothbrushes, and Walmart chartered its own ships. For longer term solutions, companies are “moving production to new suppliers or different countries and relaxing their traditional fixation with low costs.” Some goods are finalized at factories with components arriving “just in time” as freight costs skyrocket and delivery times fluctuate.
BIO-ISAC Releases Advisory to Biomanufacturers – Tardigrade: An APT attack on vaccine manufacturing infrastructure
The Bioeconomy Information Sharing and Analysis Center, or BIO-ISAC, released an advisory regarding an advanced persistent threat (APT) attack named Tardigrade. A large biomanufacturing facility was involved in a cyberattack in Spring 2021. Through the subsequent investigation, a malware loader was identified that demonstrated a high degree of autonomy as well as metamorphic capabilities. In October 2021, further presence of this malware was noted at a second facility. Due to the advanced characteristics and continued spread of this active threat, BIO-ISAC made the decision to expedite this threat advisory in the public interest. Analysis continues, and updates will be released on isac.bio as further details are made available. At this time, biomanufacturing sites and their partners are encouraged to assume that they are targets and take necessary steps to review their cybersecurity and response postures.
Biosecurity Diplomacy Workshop for Young Scientists from the Global South
The United Nations Office for Disarmament Affairs (UNODA) Geneva Branch and the Implementation Support Unit (ISU) of the Biological Weapons Convention (BWC) are delighted to open the call for applications for the third edition of Biosecurity Diplomacy Workshop for Young Scientists from the Global South. The workshop is taking place in the framework of European Union Council Decision 2019/97/CFSP in support of the BWC.
The global norm against biological weapons cannot be maintained without youth voices being included in the multilateral discussions taking place in the framework of the BWC. As fast-paced innovation in biotechnologies raises global implications for biosecurity, the young scientists of today will be on the forefront of tomorrow’s collective and innovative global solutions. This vision was stated explicitly in the UN Secretary-General’s Disarmament Agenda “Securing Our Common Future”, in which youth participation is recognized as a pre-condition to achieve the Sustainable Development Goals.
The workshop is an interactive training programme aiming at informing young scientists about their critical role in biosafety and biosecurity and bolstering global capacities against the misuse of biological agents. It will allow a new cohort of up to 30 future-oriented young biosecurity specialists from the Global South to reflect on how they envision an innovative and bio-secure future in connection with the BWC.
The workshop is open to those who: are under the age of 40; are citizens of a low- or middle-income BWC State Party; have an advanced degree in the life sciences or a related discipline from a recognized university or institution; have backgrounds in other fields such as social sciences, but have a demonstrated interest in biosecurity and/or disarmament and non-proliferation; and have a strong command of written and spoken English, as the workshop will be fully conducted in English. The deadline to receive applications is 6 December 2021, midnight CET.
BWC
BWC: Report of the Meeting of States Parties
The Meeting of States Parties to the Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction was pushed to last year as a result of the COVID-19 pandemic. The Meeting was held in Geneva from 22 to 25 November 2021. An advance version of the Report of the Meeting of States Parties is available here.
Remarks to the 2021 Biological Weapons Convention Meeting of States Parties
Ambassador Bonne Denise Jenkins, Under Secretary for Arms Control and International Security, gave her remarks to the 2021 Biological Weapons Convention Meeting of State Parties. An excerpt of her statement is below:
“For the past two decades, efforts to strengthen the Convention have been treading water. Useful discussions here have led to some small steps and actions at the national level. However, States Parties have been unable to agree to more significant action. We face a biological weapons threat that is real, serious, and, in many respects, growing. Some states continue to possess sophisticated, well-established biological weapons programs, while non-state actors have shown continuing interest in acquiring BW capabilities. Additionally, widespread availability of sophisticated scientific and technological tools and methods is gradually eroding barriers to the development of biological weapons.
While COVID-19 was not the result of a biological weapon, the pandemic is a wake-up call for all of us. The astonishing human toll of the pandemic has illustrated our shared vulnerability to novel pathogens. Unprecedented efforts are now underway to strengthen international health security, but we need to address not only the latest challenge, but those that may lie ahead, whether natural, accidental, or deliberate in origin. To do so, we must strengthen the BWC, as National Security Adviser Jake Sullivan said in his November 19 statement. The status quo is neither acceptable nor up to the task. We must take action to ensure that the Convention can effectively address the challenges we face now and in the future. We cannot keep treading water.
The first step is to overcome the political impasse of the last twenty years. We envision a two-pronged approach. The Review Conference should take near-term, concrete action to strengthen the Convention and benefit States Parties. These actions include further operationalizing assistance under Article VII; establishing a voluntary fund for technical cooperation; creating a mechanism to review advances in science and technology; deepening collaborations on biosafety and biosecurity; staffing the Implementation Support Unit to carry out these roles; and enabling more agile decision making. The second way forward is for Review Conference to also take steps to address the harder issues. It should establish a new expert working group to examine possible measures to strengthen implementation of the Convention, increase transparency, and enhance assurance of compliance. Such an effort should consider both advancements in science and technology as well as changes in the nature of the threat. As we are all acutely aware, a great deal has happened in the last two decades. It could be useful to build on some approaches suggested in past discussions, but our efforts should not be defined by them.”
Read her full statement here.
Statement to the Biological Weapons Convention Meeting of States Parties United Nations Geneva, 22 November 2021
At the Meeting of State Parties in Geneva, Switzerland, Dr. Gregory Koblentz, Director of the Biodefense Graduate Program, presented remarks drafted by himself and Dr. Filippa Lentzos from the Department of War Studies and Centre for Science & Security Studies at King’s College London. Following is an excerpt from the statement:
“One of the most politicised aspects of COVID-19 has been the question of how the pandemic started. One theory is that the virus spilled over naturally from animals to humans. Another theory is that it originated from scientific research where the virus accidentally escaped from a laboratory or scientists were infecting during fieldwork when they were collecting viral samples from bats.
It is likely we will never know the answer with any real level of confidence. We are now nearly two years into the pandemic and we’ve still not had a credible international investigation. Unfortunately, there are no signs that we will get one any time soon either. But what we do know is that it is possible to produce biological weapons that are worse than COVID-19. And we do know that dangerous viruses can escape from many labs around the world.
Dangerous viruses have been created in labs during the course of regular scientific research for many years now.
Only a handful of countries with BSL4 labs have oversight or regulatory policies in place for dual-use research. This means that the vast majority of countries with BSL-4 labs do not have specific oversight of high-risk gain-of-function research that has been a central feature in the debate on COVID-19’s origin.
We emphatically support the joint NGO statement’s call for consistent implementation of international standards on appropriate biorisk management practices, especially in laboratories working with high-risk zoonotic pathogens with pandemic potential.”
Read the full statement here.
Statement by National Security Advisor Jake Sullivan on the US Approach to Strengthening the Biological Weapons Convention
COVID-19 was a wake-up call for humanity. It revealed the devastating impact of infectious disease on our health and our societies. It also uncovered our shared vulnerability to catastrophic biological events and the lost lives, economic downturn, and global destabilization that they can cause. As we work to end the COVID-19 pandemic, we must simultaneously recognize that biological risks are growing. We face an increased threat of naturally occurring emerging diseases, as well as the potential for laboratory accidents and intentional misuse of life sciences and biotechnology. For these reasons, it is vital for us to work together – across the health, security, and development sectors – to enhance biopreparedness, biosafety, and biosecurity globally, and to reinforce the norm against the development and use of biological weapons.
The United States has made it clear that the weaponization of biological agents and toxins is unacceptable. Unfortunately, we are concerned that some nations still possess biological weapons programs, while other nations as well as nonstate actors seek to acquire them. We are therefore determined to strengthen and revitalize the Biological Weapons Convention (BWC). As we look to the Ninth Review Conference, we urge all countries to take seriously the threat of biological weapons, and for the Review Conference to overcome differences and take urgent steps to guard against the development and use of biological weapons. We must explore novel measures to promote implementation, increase transparency, and enhance compliance; measures that address the biological weapons threat of today — and tomorrow. This will be challenging work; success will require delegations to break out of old all-or-nothing mindsets and build new habits of constructive cooperation. We must demonstrate, to the world and to each other, that our shared efforts are about achieving real-world results. That is why the United States will also be proposing immediate action at the Review Conference on a number of practical measures that will build capacity to counter biological threats and benefit BWC members. The United States is committed to working with all States Parties to strengthen the BWC, and with all responsible nations to end the development of biological weapons and the threat they pose. Through collective action to counter all manner of biological threats – naturally occurring, accidental, and deliberate – together we can achieve global health security for everyone, everywhere.
ALL THINGS COVID-19
Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis
The objective of a new study published in The BMJ was to review the evidence on the effectiveness of public health measures in reducing the incidence of covid-19, SARS-CoV-2 transmission, and COVID-19 mortality. The study was designed as a systematic review and analysis, which included observational and interventional studies that assessed the effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality. The main outcome measure was incidence of covid-19. Secondary outcomes included SARS-CoV-2 transmission and covid-19 mortality. DerSimonian Laird random effects meta-analysis was performed to investigate the effect of mask wearing, handwashing, and physical distancing measures on incidence of COVID-19. Pooled effect estimates with corresponding 95% confidence intervals were computed, and heterogeneity among studies was assessed using Cochran’s Q test and the I2 metrics, with two tailed P values. 72 studies met the inclusion criteria, of which 35 evaluated individual public health measures and 37 assessed multiple public health measures as a “package of interventions.” Eight of 35 studies were included in the meta-analysis, which indicated a reduction in incidence of COVID-19 associated with, mask wearing, and physical distancing. Owing to heterogeneity of the studies, meta-analysis was not possible for the outcomes of quarantine and isolation, universal lockdowns, and closures of borders, schools, and workplaces. The effects of these interventions were synthesized descriptively. This systematic review and meta-analysis suggests that several personal protective and social measures, including handwashing, mask wearing, and physical distancing are associated with reductions in the incidence covid-19. Public health efforts to implement public health measures should consider community health and sociocultural needs, and future research is needed to better understand the effectiveness of public health measures in the context of COVID-19 vaccination. Read the article here.
The Government’s Preparedness for the COVID-19 Pandemic: Lessons for Government on Risk Management
The scale and nature of the COVID-19 pandemic and the government’s response are without precedent in recent history. Many people have died, and many lives, families and businesses have been adversely affected. By the end of July 2021, the estimated lifetime cost of measures announced as part of the government’s response was £370 billion. Like many other governments across the world, the UK government was underprepared for a pandemic like COVID-19. It will need to learn lessons from its preparations for and handling of whole-system risks, which will include making judgements on what level of preparations is appropriate.
The Cabinet Office, through its Civil Contingencies Secretariat (CCS), is responsible for coordinating the government’s planning for, and response to, major emergencies. Individual departments and other public sector organizations are responsible for identifying and managing risks in line with their desired risk appetite, including relevant national risks allocated to them by the Cabinet Office. For example, the Department of Health & Social Care is responsible for planning for the health and social care impacts of health-related risks. All departments are responsible for planning for emergencies that would have significant consequences in their areas of remit.
A new report sets out the UK government’s risk analysis, planning, and mitigation strategies prior to the arrival of the COVID-19 pandemic, with the aim of drawing out wider learning for the government’s overall risk management approach. It does not cover local-level risk planning, wider aspects of resilience planning or top-level disaster response procedures. It also does not cover the government’s response to COVID-19 or how prepared it was for subsequent waves of the pandemic.
This pandemic has exposed a vulnerability to whole-system emergencies – that is, emergencies that are so broad that they engage the entire system. Although the government had plans for an influenza pandemic, it did not have detailed plans for many non-health consequences and some health consequences of a pandemic like COVID-19. There were lessons from previous simulation exercises that were not fully implemented and would have helped prepare for a pandemic like COVID-19. There was limited oversight and assurance of plans in place, and many pre-pandemic plans were not adequate. In addition, there is variation in capacity, capability and maturity of risk management across government departments.
The pandemic has highlighted the need to strengthen the government’s end‑to‑end risk management process to ensure that it addresses all significant risks, including interdependent and systemic risks. This will require collaboration on risk identification and management not only across government departments and local authorities, but also with the private sector and internationally. For whole‑system risks the government needs to define its risk appetite to make informed decisions and prepare appropriately so that value for money can be protected. The pandemic has also highlighted the need to strengthen national resilience to prepare for any future events of this scale, and the challenges the government faces in balancing the need to prepare for future events while dealing with day-to-day issues and current events. Read the report here.
Experimental Chewing Gum Reduces Virus in Saliva
An experimental chewing gum containing a protein that “traps” coronavirus particles could limit the amount of virus in saliva and help curb transmission when infected people are talking, breathing or coughing, researchers believe. The gum contains copies of the ACE2 protein found on cell surfaces, which the virus uses as a gateway to break into cells and infect them. In test-tube experiments using saliva and swab samples from infected individuals, virus particles attached themselves to the ACE2 “receptors” in the chewing gum. As a result, the viral load in the samples fell by more than 95%, the research team from the University of Pennsylvania reported in Molecular Therapy. The gum feels and tastes like conventional chewing gum, can be stored for years at normal temperatures, and chewing it does not damage the ACE2 protein molecules, the researchers said. Using gum to reduce viral loads in saliva, they suggest, would add to the benefit of vaccines and would be particularly useful in countries where vaccines are not yet available or affordable.
PREPARING FOR THE NEXT PANDEMIC
The World Together
In a consensus decision aimed at protecting the world from future infectious diseases crises, the World Health Assembly agreed to kickstart a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.
The Health Assembly met in a Special Session, the second-ever since WHO’s founding in 1948, and adopted a sole decision titled: “The World Together.” The decision by the Assembly establishes an intergovernmental negotiating body (INB) to draft and negotiate a WHO convention, agreement, or other international instrument on pandemic prevention, preparedness and response, with a view to adoption under Article 19 of the WHO Constitution, or other provisions of the Constitution as may be deemed appropriate by the INB.
Article 19 of the WHO Constitution provides the World Health Assembly with the authority to adopt conventions or agreements on any matter within WHO’s competence. The sole instrument established under Article 19 to date is the WHO Framework Convention on Tobacco Control, which has made a significant and rapid contribution to protecting people from tobacco since its entry into force in 2005.
Under the adopted decision, the INB will hold its first meeting by 1 March 2022 (to agree on ways of working and timelines) and its second by 1 August 2022 (to discuss progress on a working draft). It will also hold public hearings to inform its deliberations; deliver a progress report to the 76th World Health Assembly in 2023; and submit its outcome for consideration by the 77th World Health Assembly in 2024.
World Commits to A Pandemic Response Pact: What’s Next
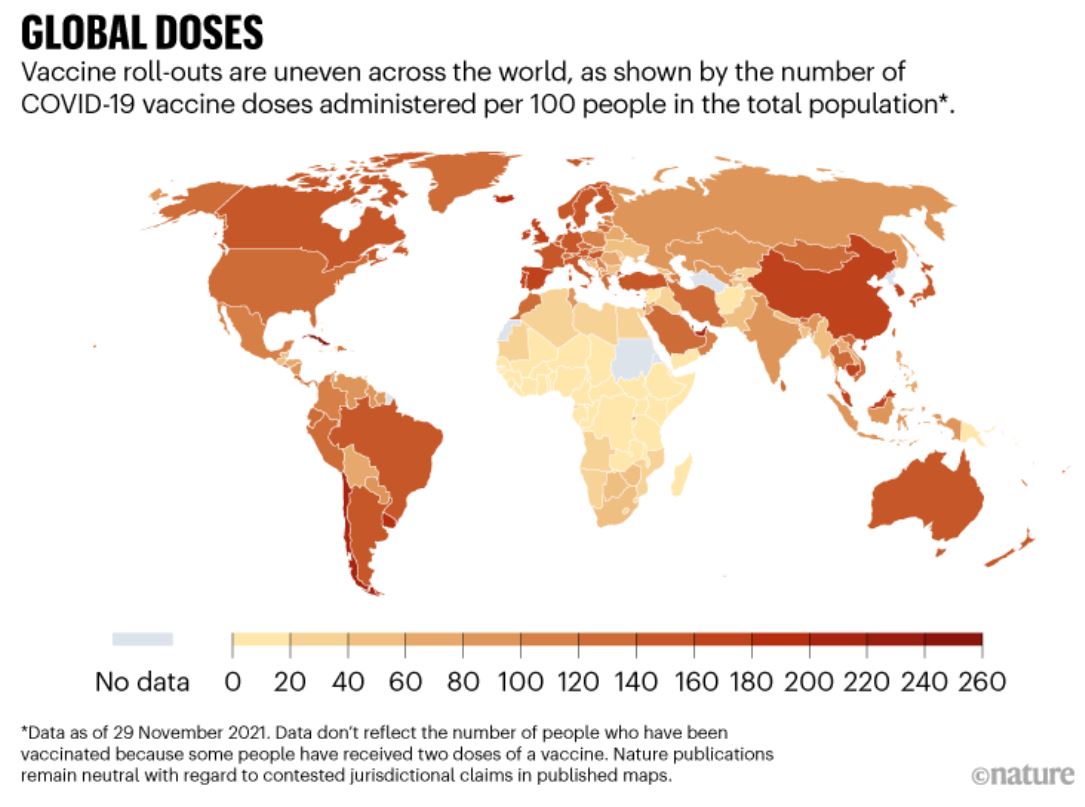
As researchers scrambled this week to learn more about Omicron, the latest SARS-CoV-2 coronavirus variant of concern, world leaders met to negotiate a way of ensuring that a crisis on the scale of the COVID-19 pandemic never happens again. The biggest decision made at the assembly is to collectively develop an accord, agreement or other ‘new instrument’ to govern pandemic response, including ensuring the equitable distribution of diagnostics, drugs and vaccines. A measure outside of the IHRs is helpful, experts say, because those regulations do not oversee vaccines and other means of fighting pathogens.
International accords — or other treaty-adjacent frameworks — typically take years to become reality, and the process for this one is expected to continue until at least 2024. The pivotal decision by the WHO’s 194 member states at this assembly to move forward with a “new instrument” marks the first step. The European Council’s Michel has said that a treaty would be a prime way to ensure the equitable distribution of vaccines and other medical countermeasures, such as protective equipment and diagnostic tests. One way to coax wealthy countries to share goods might be to link the action with sharing data, says Suerie Moon, a global health researcher at the Graduate Institute for International and Development Studies in Geneva.
Revisions to the IHRs will probably be debated at the World Health Assembly meeting next May, and amendments might even be adopted by the end of next year. But a pandemic accord or other such tool will take at least another three years.
Global and Community Health Faculty Member Shares Insight on Pandemic Preparedness in the Middle East in a New Publication
Amira Roess, professor in the College’s Department of Global and Community Health, says that while several Middle Eastern countries had preparedness plans in place prior to the COVID-19 pandemic, the region’s response shows that the implementation plans remain underdeveloped and under-resourced.
In “How Can the Middle East Better Prepare for the Pandemics of the Future?”, Roess notes that while the COVID-19 pandemic highlighted the global economic toll of emerging highly infectious pathogens, it has not yet resulted in long-lasting or meaningful investments in public health systems. She advocates for significant investments over the next five years in the region’s public health system workforce and strategic technological enhancements.
“Without thoughtful, long-term investment in public health preparedness, the mistakes of the past will be repeated,” Roess writes.
Roess’s piece is a chapter in Thinking MENA Futures from the Middle East Institute’s Strategic Foresight Initiative. The publication maps out possible futures for the Middle East and North Africa (MENA) region by drawing insight on key issues and trends from experts. The publication covers everything from economic development and the future of work to climate change adaptation and public health.
Roess is a nonresident scholar at the Middle East Institute, a nonpartisan think tank providing insight and policy analysis on matters in the Middle East. Thinking MENA Futures is available on the institute’s website.
New NTI | bio Report Recommends Actions to Prevent and Respond to High-Consequence Biological Threats
A new NTI | bio report was released on the margins of the Biological Weapons Convention Meeting of States Parties, “Strengthening Global Systems to Prevent and Respond to High-Consequence Biological Threats,” offers actionable recommendations for the international community to bolster prevention and response capabilities for high-consequence biological events.
The report, written by NTI | bio Senior Fellow Dr. Jaime M. Yassif, Dr. Kevin P. O’Prey, and Christopher R. Isaac, summarizes key findings and recommendations from a March 2021 tabletop exercise on high-consequence biological threats, jointly hosted by NTI and the Munich Security Conference. This report, and the exercise that informed it, are the third in a series of collaborations between NTI and the Munich Security Conference—which have focused on reducing global catastrophic biological risks and building stronger systems for pandemic prevention and response.
The 2021 tabletop exercise included 19 senior leaders and experts from across Africa, the Americas, Asia, and Europe with decades of combined experience in public health, biotechnology industry, international security, and philanthropy. Exercise participants were asked to engage with a fictional scenario that portrayed a deadly, global pandemic involving an unusual strain of monkeypox virus that spread globally over 18 months. Ultimately, the scenario revealed that the initial outbreak had been caused by a terrorist attack using a pathogen engineered in a laboratory with inadequate biosafety and biosecurity provisions and weak oversight. By the end of the exercise, the fictional pandemic resulted in more than three billion cases and 270 million fatalities worldwide.
The report authors developed a set of concrete recommendations for the international community based on the key findings from the exercise discussion. The recommendations include:
- Bolster international systems for pandemic risk assessment, warning, and investigating outbreak origins
- Develop and institute national-level triggers for early, proactive pandemic response
- Establish an international entity dedicated to reducing emerging biological risks associated with rapid technology advances
- Develop a catalytic global health security fund to accelerate pandemic preparedness capacity building in countries around the world
- Establish a robust international process to tackle the challenge of supply chain resilience
Read the report here.
EVENTS
2021 Global Health Security Index: Advancing Collective Action and Accountability Amid Global Crisis
COVID-19 continues to disrupt lives and livelihoods, stress health systems, and exhaust social protections and government budgets—and it will not be the last global health emergency the world will face. The need for durable national health capacities and political and social environments that foster effective prevention and response measures has never been clearer.
Join the Nuclear Threat Initiative and the Johns Hopkins Center for Health Security for the launch of the 2021 Global Health Security Index on 8 December 2021 at 9 AM EST. The GHS Index is a comprehensive assessment that provides a benchmark for capacities to prevent, detect, and respond to epidemics and pandemics across 195 countries. Register here.
The Athena Agenda: Executing the Apollo Program for Biodefense
The Bipartisan Common on Biodefense published a baseline report in 2015, A National Blueprint for Biodefense: Leadership and Major Reform Needed to Optimize Efforts, which warned that the United States was inadequately prepared for biological threats. Six years later, the US experience with COVID-19 continues to validate our original findings. The Commission’s January 2021 report, The Apollo Program for Biodefense: Winning the Race Against Biological Threats, details an ambitious goal-directed program to develop and deploy the technologies needed to defend against all biological threats, empower public health, and prevent pandemics within just ten years. Since the release of this report, the pandemic continues to cause devastation throughout the United States and the world. Likewise, the risk of an accidental or deliberate release of even deadlier pathogens continues to rise. The past year has only emboldened the idea that we cannot let a pandemic like the one we are facing, or something worse, ever happen again.
The Commission will convene an in-person meeting, The Athena Agenda: Executing the Apollo Program for Biodefense, to provide a better understanding of ongoing federal efforts to implement The Apollo Program for Biodefense, the role of the private sector in implementing The Apollo Program for Biodefense, how the public and private sectors can fully implement The Apollo Program for Biodefense within ten years. Register here.