Sally Huang is a Ph.D. candidate in the Biodefense Program at George Mason University researching the use and adoption of environmental decontamination technologies (EDT) in healthcare settings. She has a professional background in biomedical sciences, science policy, biodefense, public health, CWMD, and global health and works in the field of countering threat reduction.
In healthcare settings where infection control is paramount, far-UVC light presents a transformative opportunity to enhance patient and staff safety by continuously reducing airborne pathogen transmission. Emitting ultraviolet light at 200-235 nanometers [nm] that is both germicidal and safe for human exposure, far-UVC offers a promising solution for mitigating the spread of respiratory diseases in high-risk environments such as hospitals, clinics, and long-term care facilities. As the latest addition to a broader suite of environmental decontamination technologies (EDT)—including UV-C robots, hydrogen peroxide vapor systems, and HEPA filtration—far-UVC represents a novel approach with unique potential for continuous use in occupied spaces. Far-UVC technology has found utility across multiple sectors, including the food and beverage, water treatment, and pharmaceutical manufacturing. Among its earliest and most impactful applications is its role in addressing antimicrobial resistance (AMR) and reducing healthcare-associated infections (HAIs), which are responsible for nearly 100,000 deaths annually in the U.S.—a figure that has risen in the wake of the COVID-19 pandemic. Scientific research has demonstrated its efficacy in deactivating viruses and bacteria in the air while ongoing studies continue to support its safety for use in occupied spaces. Despite this potential, the adoption of far-UVC in healthcare still faces multiple barriers, slowed by limited public health innovation and scientific and technical analysis, regulatory uncertainty, absence of standardized safety and performance guidelines, and inconsistent implementation strategies. Effective implementation will require careful planning around far-UVC systems that are well designed, installed, and maintained to ensure reliable performance in complex healthcare environments. Taken together, these public health, scientific, regulatory, and logistical considerations underscore both the areas in need of development and the vital role that far-UVC could play in advancing infection control in healthcare settings.
Blueprint Biosecurity is a nonprofit, multidisciplinary institute dedicated to achieving pandemic prevention and mitigation through innovative research, actionable roadmaps, and practical tools. The group works at the intersection of science, technology, and policy to address emerging biological threats, improve biosafety and biosecurity standards, and inform governance of healthcare technologies and tools. Their efforts aim to ensure that life science advances are developed and applied responsibly. As part of this mission, they published a report titled Blueprint for Far-UVC report, which provides a comprehensive overview of the current state and future potential of far-UVC systems as a scalable intervention for reducing airborne disease transmission. Drawing on the latest scientific research, policy analysis, and implementation strategies, the report is a strategic roadmap aiming to guide decisionmakers, researchers, industry stakeholders, and public health officials in understanding how far-UVC can be safely and effectively integrated into shared indoor environments. As the world grapples with the ongoing threat of pandemics and seeks resilient infrastructure solutions, this report is significant for its clear articulation of far-UVC’s capabilities, the regulatory and technical challenges to overcome, and the strategic roadmap it proposes to advance this technology and facilitate widespread acceptance and adoption. The report positions far-UVC not as a speculative innovation, but as a near-term, actionable tool in the global effort to improve public health.
The Blueprint for Far-UVC report outlines ten key recommendations to guide the safe, effective, and equitable deployment of far-UVC technology, particularly in settings where the risk of airborne disease transmission is high. These recommendations are organized around core-domains—scientific research priorities, safety and consensus standards, and long term research and implementation strategy—each reflecting the multifaceted considerations necessary for scaling a novel health intervention. Alongside listing technical specifications, the report frames each recommendation as part of a broader system change, where scientific validation, regulatory clarity, and operational readiness must align.
The recommendations begin with calls to strengthen the scientific evidence base, urging continued investment in research to further validate far-UVC’s long-term safety and efficacy in real-world conditions. This is followed by a focus on developing exposure guidelines and safety standards, which the report identifies as critical bottlenecks preventing broader adoption in healthcare settings. Without formal exposure limits or unified product standards, hospitals and other high-risk facilities lack the regulatory confidence needed to deploy the technology at scale. The report also emphasizes the importance of cross-sector collaboration, recommending coordinated efforts among public health officials, scientists, industry leaders, and policymakers. Additionally, it proposes a public procurement strategy to lower costs and support early implementation in settings like hospitals, nursing homes, and transportation hubs—where the public health benefit is most immediate. Other recommendations include designing for equity and accessibility, integrating far-UVC into building codes and infrastructure plans, and launching public communication campaigns to foster trust and awareness. Collectively, these ten recommendations form a comprehensive roadmap—not only for implementing far-UVC safely and effectively, but also for embedding it within a broader public health strategy. By presenting actionable steps across research, policy, engineering, and communication, the report makes a compelling case for treating far-UVC as a viable tool in the long-term fight against airborne infectious diseases.
These recommendations also pave the exploration of additional, alternative applications of far-UVC technology. As a complementary infection prevention and control (IPC) measure, far-UVC can enhance traditional strategies like ventilation, HEPA filtration, and surface disinfection by providing continuous, passive inactivation of airborne pathogens in occupied spaces. However, successful integration requires careful coordination with HVAC infrastructure, consideration of room layout and airflow patterns, and technical expertise to ensure optimal device placement and efficacy. In older hospitals or clinics with outdated mechanical systems, retrofitting far-UVC may pose engineering hurdles that necessitate customized solutions and upfront capital investment. Despite these challenges, the potential for far-UVC to reduce nosocomial infections and protect healthcare workers makes it a valuable addition to multilayered IPC strategies.
From a broader perspective, far-UVC also holds promise as a scalable tool for global health security and pandemic preparedness. As the COVD-19 pandemic underscored the critical need for non-behavioral, infrastructure-based interventions, far-UVC showed it is a promising candidate for resilient, long-term airborne disease control. As stated in the Blueprint for Far-UVC report, preliminary analyses suggest that far-UVC could prove highly cost-effective across various dimensions (e.g., settings and environmental factors). Its utility in low-resource settings could be particularly impactful, provided that affordable and easy-to-maintain devices are made available. To realize this potential globally, countries would need to develop harmonized standards, ensure equitable access, and support far-UVC deployment through global health initiatives. In doing so, far-UVC could become an essential component in a domestic and worldwide strategy to mitigate future airborne epidemics.
The Blueprint for Far-UVC report presents a strong and detailed framework for advancing this emerging technology; however, it could be strengthened by more explicitly addressing the growing challenge of AMR and HAI and the critical need to reduce HAI. For instance, the report mentions the Center for Medicare and Medicaid Services (CMS) Hospital-Acquired Condition (HAC) Reduction Program, which financially penalizes hospitals that underperform on infection control metrics by reducing their Medicare reimbursements. While this program creates a strong incentive for healthcare facilities to improve IPC practices and reduce HAIs, it lacks clarity and support mechanisms for the adoption of healthcare technologies, like far-UVC systems. Specifically, the program does not offer explicit guidance, funding pathways, or technical assistance to help hospitals evaluate, implement, and maintain advanced environmental decontamination tools. As a result, facilities may struggle to invest in or justify the use of such technologies, even when they align with the program’s overall goals of improving patient safety and reducing infection-related costs.
The report could also benefit from a broader consideration of the systemic challenges that have historically hindered the adoption of other EDT in healthcare. Although technologies like UVC disinfection robots, hydrogen peroxide vapor systems, and advanced air filtration have demonstrated strong efficacy in reducing environmental contamination and airborne pathogens, they remain significantly underutilized across healthcare settings. This limited uptake is not due to a lack of evidence regarding its efficacy, but rather stems from a complex web of barriers seen in previous healthcare technology adoption such as fragmented regulatory oversight, procurement hesitation, operational complexity, and lack of sustained funding for implementation and maintenance. Other technologies have been developed to perform the same basic decontamination purpose as far-UVC, however these technologies are not widely deployed either. Drawing on my own research into EDT use and adoption in healthcare settings, these persistent gaps suggest that far-UVC could face comparable obstacles unless a comprehensive policy framework is developed to address these factors. The Blueprint for Far-UVC report represents meaningful progress in the healthcare technology realm and may offer useful direction for policymakers aiming to advance deployment. It highlights opportunities to pair implementation with targeted funding for pilot programs, the development of accreditation pathways for healthcare technologies, and the integration of far-UVC alongside other healthcare technologies. These measures could go a long way in reinforcing and sustaining emergency preparedness well beyond the immediate context of pandemic preparedness.
Neha Suresh is a molecular biologist, biosecurity researcher, and science communicator — nsuresh.contently.com.
The Biological Weapons Convention (BWC) stands as a monument to international ambition: the first multilateral treaty to comprehensively ban an entire category of weapons of mass destruction (WMD). The treaty’s origins are deeply rooted in the horrors of 20th-century warfare, advancements in biotechnology, and the geopolitical tensions of the Cold War.
March 26, 2025 marks the 50th anniversary of the convention entering into force. This is the optimum time to re-examine the BWC’s history, the forces that shaped it, and the persistent challenges that undermine its effectiveness. The goal of this article is not to serve just as a historical exercise, but as a vital examination of our present vulnerabilities to biological threats and the future of global biosecurity.
The 1925 Geneva Protocol prohibited the use of chemical and biological weapons in war. This prohibition reflected global revulsion at the chemical atrocities of World War I. It also reflected allegations of Germany’s use of anthrax and glanders against Allied livestock during that conflict. However, the Protocol deliberately did not ban the development, production, or stockpiling of BW. This limitation was a significant flaw that allowed nations to continue pursuing biological weapons programs.
By the 1960s, advances in microbiology, such as lyophilization (freeze-drying) of pathogens and aerosolization techniques, led to the development of more stable and deployable BW, raising concerns that existing laws were insufficient. The dual-use nature of these technologies, having both peaceful and military applications, complicated efforts to distinguish legitimate scientific research from weapons development.
A pivotal shift occurred in 1969 when the U.S. unilaterally renounced bioweapons. President Richard Nixon, citing BW’s “massive, unpredictable, and potentially uncontrollable consequences” as incompatible with U.S. interests, ordered the destruction of existing stockpiles. This move, partly influenced by the success of nuclear deterrence and the impracticality of BW for strategic goals, created diplomatic space for multilateral negotiations. Initially hesitant due to suspicions of U.S. biodefense programs, the Soviet Union, as part of its strategy to engage diplomatically, gradually supported a ban, despite not intending to comply with it.
Negotiating the BWC: Drafting a “General Purpose” Treaty
In July 1969, the UK submitted a draft convention to the UN General Assembly, proposing a total ban on BW development and production. This proposal emphasized the existential risk of BW proliferation and the need for a “general purpose” treaty, distinct from the limited scope of the Geneva Protocol. The proposal gained traction through the Eighteen Nation Committee on Disarmament (ENCD), a multilateral forum that included the United States and the Soviet Union, where non-aligned states advocated for stringent verification measures. However, these demands were ultimately deferred due to Cold War tensions.
Article I of the BWC enshrines its core obligation: never under any circumstances to “develop, produce, stockpile, or otherwise acquire or retain” microbial or toxin agents for hostile purposes. While this broad language aimed to encompass emerging technologies, the BWC treaty omitted formal verification mechanisms, relying instead on Article V’s formal consultative process and Article VI’s opaque process for lodging complaints via the UN Security Council. The Soviet Union initially opposed separating chemical and biological weapons into distinct treaties and sought a single convention covering both. However, it eventually accepted a standalone Biological Weapons Convention that classified toxins under the broader “biological” umbrella.Meanwhile, the United States resisted constraints that could limit its biodefense activities..
Why did initial calls for BWC verification fail?
The inclusion of verification measures in the BWC was a point of contention from the beginning. Despite calls for verification, the Cold War rivalry prevented the inclusion of any intrusive inspection mechanism. The U.S. and USSR harbored deep suspicions that the other was secretly continuing BW programs under the guise of defensive research. The Soviets feared U.S. intelligence operations disguised as inspections, while the U.S. was concerned that a clandestine Soviet BW program would evade detection.
Entry into Force and Early Challenges
The BWC entered into force on March 26, 1975, following ratification by 22 states, including its three depositary governments (the Soviet Union, the United Kingdom, and the United States). By 2023, 188 nations had joined the Convention, though key holdouts (such as Egypt, Israel, and Syria) highlight ongoing geopolitical divides. Early adherence was bolstered by the treaty’s perceived symbolic value, but implementation lagged, with few states enacting robust national legislation to criminalize BW activities and the confidence-building measures (CBMs) suffered from inconsistent reporting.
The BWC in the 21st Century: Adapting to New Threats
The BWC faces a complex landscape in the 21st century. Rapid advancements in synthetic biology, CRISPR gene editing, and gain-of-function research have dramatically increased the dual-use risks. The proliferation of high-containment labs ( 51 BSL-4 facilities in operation worldwide) has made comprehensive monitoring more challenging.
The COVID-19 pandemic served as a brutal reminder of the devastating potential of both natural and potentially engineered pathogens. The pandemic has revitalized discussions around the BWC’s Article X, which focuses on peaceful international cooperation. Initiatives like the WHO’s BioHub Facility and the Global Partnership Against WMD’s biosecurity projects aim to better integrate the BWC with the global health framework.
Some old tensions remain. Developed nations, wary of dual-use risks, push for stronger verification and biosafety standards. Developing countries emphasize the need for equitable access to biotechnology for public health and economic development. This divide continues to hinder the BWC’s ability to effectively address both global biosecurity and scientific collaboration.
The old debates about verification have resurfaced, but progress remains elusive. In the 1990s, efforts to introduce more stringent monitoring were blocked, culminating in the U.S. rejection of a 2001 verification protocol. While the Ninth BWC Review Conference in 2022 rekindled discussions through the creation of a new Working Group, a consensus is still out of reach.
Conclusion: The BWC’s Legacy and Unfinished Agenda
The BWC stands at a critical juncture. Born from a moment of moral clarity and scientific foresight, it represents an attempt to build a shield against one of humanity’s darkest impulses. But its inherent flaws – the lack of verification and the reliance on trust – have left it vulnerable.
As biotechnology empowers more actors and makes the engineering of biological agents easier, the BWC must adapt or risk becoming obsolete. Enhanced transparency, equitable cooperation, and innovative monitoring tools are essential if the Convention is to remain relevant in an age of unprecedented biological risks. The ongoing work of the 2023-2026 Working Group offers a chance to rewrite the narrative, and to ensure that the future is not defined by the weaponization of life itself.
Gregory D. Koblentz, David Gillum, and Rebecca Moritz
October 15, 2024
On September 25, 2024, Senator Rand Paul introduced a revised version of the Risky Research Review Act (S. 4667) which was voted out of the Senate Homeland Security and Government Affairs Committee by a vote of 8-1. In a recent OpEd in STATNews, we wrote of the original bill: “this legislation threatens to cast a shadow over the future of life sciences research and slow it down.” While this revised bill contains some positive changes, it remains deeply flawed and does not represent a viable solution to the challenges posed by dual-use research. This article analyzes the good, the bad, and the ugly of the revised Risky Research Review Act and finds that the negative features outweigh the positive ones.
The Good
The revised bill contains three positive additions compared to the original: the inclusion of a biosafety expert on the Life Sciences Research Security Board, the provision for expedited review of high-risk life sciences during an emergency, and a clearer definition of high-risk research that is more closely aligned with current U.S. government policy.
The composition of the Life Sciences Research Security Board has improved slightly. In our OpEd, we wrote, “The composition of the proposed board also raises serious concerns about its ability to effectively oversee high-risk research. The board would consist of political appointees, including life scientists and national security experts, but lacks a requirement for members to have expertise in biosafety and biosecurity. This omission is critical, as effective oversight of high-risk research requires nuanced understanding and practical, hands-on experience in these areas.” The revised bill now includes one biosafety expert on the Board, in addition to the executive director, five non-governmental life scientists, and two non-governmental experts in national security. Ideally, this expert should have practical hands-on biosafety experience both implementing research policy on a daily basis as well as reviewing life science research for potential misuse and developing risk mitigation measures. The new composition of the Board is one step closer to the long-recognized and widely supported need for a multidisciplinary approach to oversight of dual-use research. For example, current guidance from Office of Science and Technology Policy is that committees at Federal funding agencies conducting reviews of dual-use research should include representatives with experience in scientific research, biosafety, biosecurity, national security, and ethics, and other relevant areas.
The revised bill, however, does not address a problem we raised regarding how the bill’s conflict of interest provisions could affect the composition of the board: “The bill’s provisions regarding conflicts of interest defined too broadly could also disqualify many well-qualified individuals from serving on the board. It would exclude scientists with experience conducting high-risk research, which could result in a board lacking the necessary knowledge, expertise, and skills to make informed decisions about the risks and benefits of life sciences research, thereby undermining its effectiveness and credibility.”
Another good addition to the bill is a provision, in section 7906(d), for expedited review of high-risk life sciences research during a public health emergency or to address a specific national security concern. This was a necessary addition given the legislation’s 120-day timeline for reviewing and approving research proposals involving high risk life sciences research.
The revised bill also more clearly defines the scope of what it considers “high risk life sciences research” and this definition is in closer alignment with the 2024 United States Government Policy for Oversight of Dual Use Research of Concern and Pathogens with Enhanced Pandemic Potential (also known as the 2024 DURC/PEPP Policy), but the scope of high-risk research still has important ambiguities. The definition of high-risk life science research includes “gain of function” research and dual-use research of concern (DURC) involving a high-consequence pathogen (HCP), a new term of art introduced by this bill. However, the overall scope of the Risky Research Review Act is actually narrower than the 2024 DURC/PEPP Policy.
The definition of dual-use research of concern in section 7901(4) is mostly aligned with the definition of Category 1 Research in the 2024 DURC/PEPP Policy, with a few minor exceptions. The bill adds two additional experiments of concern to what constitutes DURC under the 2024 Policy: enhancing the transmissibility of a pathogen in humans (7901(4)(B)(i)(X)) and enhancing the virulence of a pathogen in humans (7901(4)(B)(i)(XI)). Since enhancing the transmissibility and virulence of pathogens are already covered under 7901(4)(B)(i)(I) and (7901(4)(B)(i)(II), respectively, it is not clear what the purpose of including these additional experiments are.
In addition, the bill includes “generate, use, reconstitute, or transfer an eradicated or extinct high-consequence pathogen” which is broader than the 2024 DURC/PEPP Policy which specifies such research with a pathogen with pandemic potential (PPP) or a previously identified pathogen with enhanced pandemic potential (PEPP). There are only three eradicated or extinct pathogens of concern—variola major, variola minor, and rinderpest. Since the generation, use, reconstitution, or transfer of variola major and variola minor are already covered by 18 US Code 175c, the 2024 DURC/PEPP Policy, and the Select Agent Regulations, the only impact of this provision is to apply the same restrictions to rinderpest, which is not considered a PPP since it does not affect humans.
The bill defines gain of function under section 7901(7) as “a research experiment that may enhance the transmissibility or virulence of a high-consequence pathogen.” The inclusion of gain of function as a separate category is redundant since the revised bill’s definition of dual-use research of concern also includes research involving the enhancement of transmissibility under 7901(4)(B)(i)(I) and 7901(4)(B)(i)(X) and enhancement of virulence in 7901(4)(B)(i)(II) and 7901(4)(B)(i)(XI).
This bill, like the 2024 DURC/PEPP Policy, covers these specified research activities when conducted in conjunction with certain pathogens. Like the 2024 DURC/PEPP Policy, the bill uses list-based and risk-based approaches to define what it considers to be a high consequence pathogen. The risk-based approach is identical to that used by the 2024 DURC/PEPP Policy to identify a PPP, namely a “pathogen that is likely capable of wide and uncontrollable spread in a human population and would likely cause moderate to severe disease and/or mortality in humans.” The list-based approach used by the bill (which is shorter than the original bill) yields a narrower list of agents subject to oversight compared to the 2024 DURC/PEPP Policy.
The list used by the revised bill includes wild-type or synthetic versions of influenza A viruses (excluding seasonal strains); sarbecoviruses, a subgenus comprised of 1 species; merbecoviruses, a subgenus comprised of four species; 11 other specific viruses; Yersinia pestis; and “a select agent or toxin, work with which poses a significant risk of deliberate misuse.” There are currently 68 agents and toxins under the Federal Select Agent Program. It is unclear what the bill means by “work with which poses a significant risk of deliberate misuse,” under what conditions research with a select agent and toxin would be trigger this provision and be considered a high-consequence pathogen, and how this definition relates to how the bill defines dual-use research of concern. If this provision is intended to subject all research with select agents, even with unmodified wild-type strains, to approval by the Board, then it belongs in the category of bad features of the bill.
Overall, the revised bill is an improvement over the original. However, the improvement is marginal and the bill is still plagued with definitional ambiguities. Overall, these positive changes are outweighed by the continued negative aspects that are retained from the original bill and are detailed in the next section.
The Bad
At its heart, this bill contains the same flawed process for reviewing high-risk life sciences research and the same excessive overreach we criticized in the original bill. As we wrote in STAT News,
“The proposed Life Sciences Research Security Board would have the unprecedented authority to veto funding for life sciences research, regardless of whether it is deemed high risk. This authority would effectively place the entire federally funded life sciences research enterprise under the board’s jurisdiction. This provision is particularly worrisome because it would allow the board to overrule agency decisions on a wide range of life sciences research, potentially including projects with minimal, or even no significant risk. Such extensive veto power could disrupt the research funding process, causing extensive delays that hamper scientific progress. This broad oversight could lead to a significant increase in the volume of research proposals subject to review by the board, further slowing down the funding process and creating bottlenecks that impede timely scientific advancements.”
Under the original and revised bills, entities that apply for Federal life sciences research funding must attest to whether their research falls into the category of “high-risk life sciences research” or not (section 7905(b)). The Federal funding agency receiving the proposal must then review these attestations and forward positive attestations to the Board for review. However, the funding agencies must also review negative attestations and “certify” that these attestations are valid. While the enforcement provisions in section 7905(g) of the revised bill are less draconian than those in the original bill, they are stiff enough that they will create a strong incentive for agencies to scrutinize every life sciences research proposal submitted to ensure that the offered attestation, positive or negative, is correct. In addition, the need to review and certify life science research proposals that are not deemed to be high risk will absorb additional resources within funding agencies. This will inevitably slow down the review and approval of all proposed life sciences research, even if it is declared not to pose a high risk.
The Board can take up to 150 days (an agency submits notification 30 days before award and the Board has 120 days to review) to render their determination on proposed high-risk research. Therefore, proposed high-risk life sciences research could be delayed for up to five months beyond the current process, assuming this new review process runs smoothly. If proposers or funding agencies categorize a broad range of life sciences research as high-risk to avoid being accused of not following the legislation, then this lengthy review process could affect a much larger volume of research beyond that which is genuinely high-risk, and it will be more difficult for the Board to review proposals based on this timeline.
The bill also gives the Board the ability to expand its jurisdiction unilaterally by changing the definition of dual-use research of concern (under section 7901(4)(B)(ii)) and expand the list of HCPs (under section 7901(8)(A)(ii)(XVII). Coupled with the lack of provisions requiring the Board to solicit public comment on proposed procedures for the high-risk life sciences proposal review process (under section 7904(c)), there is a significant risk that the Board could engage in regulatory overkill that fails to balance the risks and benefits of the dual-use research it is charged with overseeing.
A highly problematic provision of the original bill retained in the revised bill extends the jurisdiction of the Board to all life sciences research, even if it is not considered high-risk. Under section 7906(a)(2), the Board will have the authority to review all proposed research in the field of the life sciences, even if it is not designated as high-risk and determine if it should be funded or not. In section 7901(10), the revised bill defines life sciences research as the study or use of a living organism, virus, or product of a living organism, and “each discipline, methodology, and application of biology, including biotechnology, genomics, proteomics, bioinformatics, and pharmaceutical and biomedical research and techniques.” While this is a narrower definition than found the original version, it is still broad enough to provide the Board with unfettered control over the entire Federally funded life sciences research enterprise. Federal agencies spent $42.5 billion on life sciences research in 2020. In 2022, Federal agencies awarded approximately $30 billion to academic institutions for life sciences research.
The Ugly
Several features of the bill make the Board vulnerable to abuse which could have a chilling effect on a wide swathe of life sciences research that includes work on infectious diseases and the development of medical countermeasures.
Under section 7906(a)(3), the Board will have the authority to audit previously funded life sciences research that was determined not to be high-risk. The bill, under section 7905(e), also gives the Board the power to demand “any information relating to Federal funding awards for life sciences research determined necessary by the Board to provide oversight of the agency.” In addition, under 7905(h)(3), the Board may request additional information directly from an entity that has proposed or is receiving Federal funding and uses subawards or subcontractors to conduct its research. These provisions appear designed specifically to empower the Board to investigate the National Institutes of Health’s (NIH) previous decision to fund research on chimeric coronaviruses by EcoHealth Alliance at the Wuhan Institute of Virology, which was deemed by NIH not to fall within the scope of the Office of Science and Technology Policy’s Recommended Policy Guidance for Departmental Development of Review Mechanisms for Potential Pandemic Pathogen Care and Oversight (or P3CO Policy). Senator Paul has been one of the leading voices linking this research to the origin of SARS-CoV-2 and the COVID-19 pandemic.
The partisan nature of the bill is reinforced by several provisions that grant Congressional members and committees’ extensive access to the inner workings of the Board, Federal funding agencies, and research institutions that conduct life sciences research. Under section 7902(g), the Senate Homeland Security and Government Affairs Committee and the House Committee on Oversight and Accountability shall “have access to any records provided to or created by the Board.” The Board must respond to requests for information from a member of Congress within 30 days and the Board must brief the appropriate Congressional committees at least quarterly. While congressional oversight of executive agencies is both proper and necessary, the degree of congressional access and influence hardwired into the Board makes it more vulnerable to political pressure. The perception that the Board is being used as a stalking horse by political actors will undermine its legitimacy, credibility, and effectiveness.
Conclusion
Although this legislation is touted as focusing on the review of high-risk life sciences research, the Board’s authority to review all life sciences research, regardless of risk level, and veto funding agency decisions, will result in the close scrutiny of a much wider swathe of life sciences research which will likely lead to significant delays in the funding of this research. In addition, the ambiguities in its definition of high-risk life sciences research, the additional scrutiny of life sciences research that is not deemed high-risk, and the broad authority to investigate how funding agencies and institutions conduct research has the potential to have a chilling effect on the willingness of U.S. scientists to seek Federal funding for research with dangerous pathogens and for Federal agencies to fund such research. This could, paradoxically, incentivize researchers to seek funding from the private sector or foreign sources, which will exercise little to no oversight for biosafety or biosecurity. The end result could be a less dynamic, innovative, and competitive life sciences research enterprise in the United States and riskier research being conducted with less oversight.
Gregory D. Koblentz is director of the Biodefense Graduate Program at George Mason’s Schar School of Policy and Government and co-director of the Global BioLabs Initiative.David Gillum is associate vice president of compliance and research administration at the University of Nevada, Reno, an associate editor of Applied Biosafety, and co-founder of Tutela Strategies. Rebecca Moritz is co-founder of Tutela Strategies and is the immediate past president of ABSA International.
Shockingly low case counts, the Party’s Central Economic Work Conference concludes, thick smoke emanating from Beijing crematoriums, and a closed-door meeting of the National Health Commission…
Amid the endless stream of Tweets and headlines warning of a massive wave of COVID-19 deaths in China, there is no shortage of discussion about how serious the situation in the country might become. However, there has been some confusion, incomplete information, and countless questions circulating about what is known right now. We discussed the rollback of China’s Zero-COVID policies and growing problems like antiviral shortages in last week’s Pandora Report, so check there for more detailed discussion on those topics. This update aims to explain and clarify what is known about the current situation and analyze what might happen as a result of it, covering how China is counting cases and deaths, what vaccines are available in the country, critical threats the healthcare system is facing, and what this means in the current economic and political environment in the country.
The Basics
The current wave in China is being driven by BF.7, which is short for BA.5.2.1.7, a sub-lineage of the Omicron BA.5 variant (good luck remembering all that!). BF.7 is reported to transmit faster than other variants, have a shorter incubation period, and be better able to infect those who previously had COVID-19 or are vaccinated. Dr. Li Dongzeng, Chief Physician at Beijing YouAn Hospital’s Infectious Disease Department, reported late last month that BF.7 is thought to have an R0 between 10.0 and 18.6. For context, the original strain of SARS-CoV-2 had an R0 between 2.0 and 3.0 and it officially infected 68,150 people as it ripped through Wuhan in 2020, though estimates of the true case count are as much as three times that number. Given what we have discussed previously about China’s Zero-COVID policy, specifically its failed vaccine strategy, this is incredibly dangerous with many models predicting around one million COVID-19 deaths in China in the coming months. Furthermore, with the rollback of Zero-COVID restrictions, a massive, immunologically vulnerable population is likely to be quickly infected, causing national and global economic problems. This policy pivot is also likely to further complicate business for the Chinese Communist Party (CCP) as its credibility is challenged by this spread and as the likely economic and human costs it will bring come to fruition.
What’s Up with China’s Case and Death Counts?
The incredibly low case and death counts China is reporting currently have left many highly skeptical of the government’s truthfulness. For example, there were officially five COVID-19 deaths on Tuesday, December 20, and just two the day before-and zero in the two weeks prior. The government also reported shockingly low numbers of new cases throughout this week. Meanwhile, the World Health Organization reported that China has 26,878 new cases and 78 new deaths, causing some confusion online and in media reporting. So, what gives?
First-What Counts as China in These Numbers?
Regarding the WHO numbers, it is important to remember that they include Taiwan’s counts in the totals for China. While the WHO’s interactions with and stance on Taiwan made global headlines in early 2020, little has been done to address this issue. Taiwan, officially the Republic of China (ROC), initially represented China in the United Nations and its umbrella organizations. This was because China was one of the original UN member states during the organization’s creation in 1945. This predated the Chinese Communist Party’s defeat of the Kuomintang-led government of the ROC, which led to the establishment of the People’s Republic of China (PRC) and the exiling of the ROC to the island of Taiwan in 1949. The ROC (still under the leadership of Chiang Kai-shek) continued to represent China in the UN until the passage of United Nations General Assembly Resolution 2758, or the Resolution on Admitting Peking, in 1971. This resolution recognized the PRC as “the only legitimate representative of China to the United Nations,” giving the PRC its permanent seat on the UN Security Council and expelling “representatives of Chiang Kai-shek from the place which they unlawfully occupy at the United Nations and in all the organizations related to it.”
Though Taiwan has functioned as a self-ruled democracy since 1949, the PRC insists that Taiwan is a renegade province that will eventually be reunified to the rest of the country. As a result, Taiwan lacks proper representation in organizations ranging from those in the UN System to the International Olympic Committee (where it is listed as Chinese Taipei). While this might normally seem like a purely political issue between the countries, it has important implications, particularly in the context of global health. Taiwan is an excellent international player in pandemic response, as demonstrated in its work to support other countries during the COVID-19 pandemic. The WHO has been largely unresponsive, however, which many critics argue is because the PRC forces its view of Taiwan as a province of the PRC on international organizations, irrespective of the potential harm this carries in matters like international development and global health. Earlier this year, there was a movement to allow Taiwan to attend the WHO’s World Health Assembly as an observer, which had support from 13 member states, including the United States. However, this bid was rejected.
Important to also consider is that the WHO counts Hong Kong and Macao in its counts for China, whereas some data sources differentiate between them and the mainland. Hong Kong and Macao are special administrative regions (SARs) of the PRC with their executive, legislative, and judicial powers devolved from the national PRC government. These SARs are the subject of the “one country, two systems” policy in China which came about as Hong Kong and Macao were transferred to the PRC from the United Kingdom and Portugal respectively in the late 1990s. Under this policy, the SARs would continue to have their own governments and maintain functions like overseeing their own legal financial affairs, including foreign trade. This has allowed them to hold onto their distinct cultures and functions with, for example, both SARs maintaining their own currencies separate from the PRC’s renminbi. In recent years, China has aimed to reduce the independence of the SARs, taking aim at Macao’s famous casinos this year and implementing the Hong Kong National Security Law in 2022, which sharply reduced Hong Kong’s autonomy. Importantly, despite these changes, the SARs have separate healthcare systems and have implemented different policies to control COVID-19 than the mainland. As we will discuss later, this has made the SARs an attractive location for mainlanders to seek care and vaccinations. However, the point here is that it is important to take Taiwan and the SARs into consideration when looking at COVID-19 cases and deaths in China.
Daily confirmed cases and deaths in China (the mainland PRC), Hong Kong, Macao, and Taiwan from Our World in Data, which uses Johns Hopkins University’s Center for Systems Science and Engineering’s COVID-19 Data Repository. This repository counts cases and deaths by dates of reporting, not by the actual dates of tests and deaths. Furthermore, it is possible to get separate counts for each of these places on this site. Meanwhile, the WHO’s Coronavirus (COVID-19) Dashboard reports official daily counts made by countries, territories, and areas, accounting for some of the discrepancies pointed out by many.
What Does the PRC Consider a COVID-19 Death?
Irrespective of all this, the low number of total deaths in mainland China is still suspicious given the sudden policy reversals and sub-pay vaccines in the country. This is made worse by reports of funeral homes and crematoriums in the country being overrun by COVID-19 victims. For starters, the Chinese government is very strict in how it identifies a cause of death, which was a point of confusion even before this pandemic in comparing things like influenza mortality rates in the United States and China. However, it is even more important right now. China is only counting deaths from pneumonia or respiratory failure in its official COVID-19 deaths. This does not include deaths of COVID-19 patients who had pre-existing conditions, and proof like evidence of lung damage caused by SARS-CoV-2 is required for confirming COVID-19 deaths. This goes against the WHO’s guidelines and helps explain the shocking discrepancies between China and other countries’ COVID-19 death counts. During the outbreak in Shanghai earlier this year, many also claimed that their elderly family members who tested positive for COVID-19 and then later died were not included in the city’s official COVID-19 death count if they had underlying diseases, for example. Essentially this means that, even without overtly concealing numbers, China will always have a lower mortality rate than countries that count deaths where COVID-19 was a factor as COVID-19 deaths.
What About the Case Counts?
Okay, so it isn’t a COVID-19 death if a person has any kind of underlying condition or did not clearly die of pneumonia or respiratory distress after testing positive for COVID-19–but why are China’s case counts still so low? In the last two weeks, China has abandoned its mass testing strategy completely and even gone so far as to stop counting asymptomatic COVID-19 cases. It has also slashed central quarantine requirements, further reducing opportunities to accurately count cases. In May this year, as hundreds of millions were forced into lockdowns, the government ordered all cities with more than 10 million people to implement routine testing requirements and to ensure that testing facilities were available within a fifteen-minute walk from anywhere in the city. Places like malls, grocery stores, and restaurants required people to show a negative PCR test from less than 48 or 72 hours ago in order to enter, meaning that people were constantly testing even if their city, neighborhood, or building were not locked down.
Large scale mandatory testing was also mandated when cities entered lockdowns after cases were detected. For example, when Shanghai shutdown in March this year, the city tested all 26 million residents as it kept them all at home or in public quarantine centers if they were positive. The disease spread widely again this fall, prompting lockdowns across the country in an effort to control outbreaks ahead of the National Congress of the Chinese Communist Party, further demonstrating that the Party’s Zero-COVID strategy was not working well even with mass testing requirements.
In mid-November, as cases soared in Guangzhou and Chongqing and discontent rose across the country, the National Health Commission announced its 20 rules for optimizing Zero-COVID, which included relaxation of quarantine measures. This coincided with cities like Shijiazhuang, Yanji, and Hefei announcing they would end their mass testing programs. Later, cities like Beijing and Shenzhen relaxed their requirements for negative tests to use public transportation on December 3, which came before the total abandonment of mass testing just days later following the State Council’s announcement of its ten-point plan on December 7. Xinhua News, an official state media outlet, reported on December 7 that the new rules indicate that, “Apart from nursing homes, medical institutions, primary and secondary schools, kindergartens and other special places, people will no longer be required to provide negative nucleic acid test results and undergo health code checks to access public venues or travel to other regions.”
Furthermore, the ten-point plan’s changes in quarantine policies and determination of high/low risk areas are impacting overall case counts. While the previous 20 rules from November cut down central quarantine facility requirements, ended many mass testing requirements, and changed testing and arrival procedures for international flights, the new ten-point plan totally cut central quarantine requirements for mild and asymptomatic cases. It also changed requirements for close contacts to just five days of home quarantine as well, in lieu of being taken to a central facility. While these new requirements are helpful in that people should not be yanked away for an unknown amount of time because they are considered a close contact, these new changes also mean it is not really possible to have a reasonable understanding of the full extent of COVID-19’s spread in the country. While other countries have dealt with similar issues as at-home testing became more common, this is a much more complicated problem as China faces a winter of overwhelming case counts.
However, as we discussed on Sunday, provinces are introducing rollbacks at different paces. Now we are also seeing cities reintroducing stricter measures on their own, with Shanghai ordering schools and childcare facilities to close this Monday as cases climb. This has created a confusing patchwork of different policies and requirements, further adding to the chaos unfolding as China exits Zero-COVID. As we mentioned last time, CSIS has a helpful map tracking where provinces are at in terms of rolling back restrictions, though it is still hard to keep track of how individual cities are responding as the situation progresses.
Finally, in perhaps the most shocking change, many in China are being encouraged to go to work still even if they are positive for COVID-19. Earlier this month, with some hospitals reporting as many as 80% of their staff were infected, healthcare workers were encouraged or required to still come into work in order to keep up with demand. Now several local governments in China have asked workers to continue going to work even if they are sick in what many view as a warning of the coming economic problems that will be discussed later in this post. These complete 180° changes are simultaneously removing virtually all precautions while also overtly encouraging further infections by encouraging or requiring those who are sick to continue going around others.
Announcement of Chengdu’s new “2+3” requirements for people arriving to the city. In this scheme, arrivals will take one nucleic acid test on arrival and one on their first day at a quarantine hotel. They will spend just two days in quarantine before staying home for three days afterwards, in contrast to the 7+3 and 5+3 arrangement previously in place. For context, Chengdu, the capital of Sichuan province, locked down entirely for four days just in September to test its 21.2 million residents after 157 cases were detected.
A Glimpse Into What’s Actually Happening?
Despite the impossibly low official counts presenting by the government, a closed-door meeting of the National Health Commission reportedly offered a much better look into how many are currently infected. Reports claim that Sun Yang, Director of the Chinese Center for Disease Control and Prevention, informed the commission that at an estimated 37 million people, or about 2.6% of the population, are thought to be recently infected. Estimates from this meeting also indicate that about 248 million Chinese were infected between December 1 and 20, making the cumulative infection rate about 17.56%. The provinces with the high single-day new infection rates are Sichuan, Anhui, Hubei, Shanghai, and Hunan. Perhaps most shockingly, both Sichuan and Beijing are thought to have infection rates over 50%. Finally, infections have spread more rapidly in the Jingjinji Metropolitan Region (the megalopolis of Beijing-Tianjin-Hebei), the Chengdu-Chongqing region, Hubei and Central China. In contrast, the Yangtze River Delta (another megalopolis incorporating Shanghai, China’s most populous city), the Pearl River Delta (yet another megalopolis in the Guangdong–Hong Kong–Macau Greater Bay Area), and the Northwest and Northeast regions of the country are less impacted thus far.
Post from popular Twitter account sharing Chinese social media posts and trends, Teacher Li is Not Your Teacher, featuring posts by netizens discussing the National Health Commission Meeting.
Though these reports indicate health officials believe Beijing is past the peak of this phase, this is still very clearly just the beginning of this disaster. Shanghai has already ordered schools to shutdown in anticipation of growing case counts, in contrast to Beijing (which rolled back essentially all of its COVID-19 policies) and Chengdu, the capital of Sichuan province and the producer of the 2+3 quarantine poster above. As we will discuss further down in this post, this situation is likely to get far worse as the disease continues to spread in other major metropolitan centers and, eventually, across rural regions of the country, especially with the country’s subpar vaccines and the approaching holiday travel season.
Don’t Shoot the Messenger(RNA): China’s COVID-19 Vaccine Problem
Earlier in the pandemic, China claimed that it was nearing production of a domestically-produced mRNA vaccine for COVID-19 (even going so far as to announce the construction of a facility to manufacture ARCoVax/AWcorna in late 2020) and that it would approve the mRNA vaccine from Pfizer/BioNTech. Today, AWcorna only has emergency use approval in Indonesia, and the only people who have access to the Pfizer/BioNTech shot in China are German expats. China’s vaccination campaign has instead depended on two domestically-produced inactivated offerings-Sinopharm BIBP and CoronaVac. The country did recently approve and rollout CanSino Biologics’ aerosol offering, Convidecia Air, a viral vector vaccine growing in popularity as more Chinese seek out booster doses.
In mid-2021, the WHO approved the initial two offerings for emergency use based on limited clinical-trial data indicating that CoronaVac was about 51% effective while Sinopharm was about 79% effective. This was alright relative to the 63% efficacy reported for AstraZeneca’s viral-vector vaccine, but it was not as effective as the 90%+ reported for the Pfize-BioNTech and Moderna mRNA offerings. Nature News explained the initial criticism of China’s vaccines, writing “Both the Chinese vaccines are inactivated vaccines, which use killed SARS-CoV-2 virus. Researchers say this type of vaccine seems to be less potent because it triggers an immune response against many viral proteins. By contrast, mRNA and viral-vector vaccines target the response to the spike protein, which is what the virus uses to enter human cells.”
These numbers sound okay, especially with a high number of fully-vaccinated individuals in the country, but these efficacy rates were for the original strain found in Wuhan in 2020 and it has been several months since most people received their last dose of vaccine. 90.3% of the population has received the entire initial protocol, but, as of December 20, just 60.5% of the population has received a booster dose. Worse, those numbers shrink to 65.8% and 40% respectively for those over the age of 80 as of November. During Hong Kong’s outbreak earlier this year, similar hesitancy in elderly people (just 20% were vaccinated at the start of the outbreak in February) contributed to widespread death in the city’s nursing facilities. China announced in late December it would push to vaccinate those over the age of 60, though this is likely too little too late now, particularly given Chinese vaccines’ even more limited efficacy against Omicron and its sub-variants.
Finally, as was hinted previously, Macao and Hong Kong have become popular destinations for mainlanders throughout the pandemic, in large part because Pfizer/BioNTech’s mRNA offering is available in the special administrative regions. The SARs have also largely sold out of cold and flu medications and painkillers after the rollback of Zero-COVID on the mainland as people rush to find these supplies where they could.
Why Isn’t There a Vaccine Mandate?
This issue naturally leads to questions of why the government hasn’t just mandated vaccines already, even if the ones they can offer are not as effective as the mRNA offerings in the West. A vaccine mandate intuitively makes sense at first look, especially as much of the discourse about China’s handling of COVID-19 in the early days of the pandemic centered on the potential benefits of authoritarian rule in pandemic response. However, if it isn’t clear yet, China is playing a unique game and even its brand of authoritarianism is not always black-and-white.
There were attempts to create a mandate, with the Beijing Municipal Health Commission announcing one this summer, for example. Dr. Yangzhong Huang at the Council on Foreign Relations explained the announcement in June, writing “On July 7, Li Ang, the deputy head of Beijing Municipal Health Commission (BMHC) announced that beginning on July 11, those who had not received COVID-19 vaccines would be denied access to public venues including libraries, museums, and cinemas. The mandate also stated that those elderly who live in military and civilian retirement and nursing homes, as well as their visitors, be fully vaccinated.”
Chinese social media was lit up with backlash over the mandate and concerns that citizens’ informed consent was being compromised. Others directly asked the municipal government to reverse the policy, which ultimately did happen the very next day on July 8. Many around the world touted this as a victory for the people, but this is bizarre event points to the difficulty in understanding China’s health policies and to a complicated vaccine hesitancy more than a purely anti-vaccine sentiment. As Huang points out, this reversal came in a city where 98% of the residents were fully vaccinated. Furthermore, that explanation does not explain why the government reversed its policy on vaccines but not on other also unpopular measures like central quarantining. This reversal was also in response to social media posts over the course of a day so, while local governments in China do make similar policy reversals in the face of opposition movements, this usually takes much more time and is the result of backlash that is much more serious in nature. While Huang’s piece focuses on fragmented authoritarianism in the CCP and friction between leaders who supported Zero-COVID and mass vaccination, it also offers very important context for understanding vaccine hesitancy in China.
While there are younger people in China who have openly avoided getting vaccinated for COVID-19, this problem is concentrated in the elderly population. Again using the example of Hong Kong this year, 20% were vaccinated at the start of the outbreak in February, in sharp contrast to the more than 60% in that same group who were vaccinated for seasonal influenza. For reasons discussed earlier in this post, it makes sense for Hong Kong’s elderly to be hesitant to take a vaccine offered by the PRC’s government. However, these low rates were true despite the Pfizer/BioNTech mRNA vaccine being available.
While some point to the initial focus on essential workers as a likely reason why vaccination rates lag in China’s elderly population, a history of scandal is likely in large part to blame. For example, in 2018, Changchun Changsheng Life Sciences was fined ¥ 9.11 billion (about $1.32 billion at the time) after an investigation by the National Medical Products Administration found the company in violation of eight drug regulations. This kind of punishment was at the very least rare and came after some had severe reactions to the company’s rabies vaccine. The incident led many netizens to express their distrust in the country’s pharmaceutical industry, prompting calls from the likes of Xi Jinping and Li Keqiang for severe punishment for the company. However, the effects of this and similar events seem to have stuck around.
John Ruwitch discussed this issue recently in a piece for NPR, writing “It wasn’t always like this, according to Mary Brazelton, an expert in the history of science and medicine in China at the University of Cambridge. In the months after the Communist takeover in 1949, the Chinese government launched several successful vaccination campaigns, taking on smallpox, tuberculosis, diphtheria and other diseases.”
He continues, “If you look at earlier periods in the People’s Republic of China’s history…what you see is in some ways almost the opposite in terms of really strong vaccination programs that work quite hard to convince people, particularly elderly people, to receive vaccines against infectious diseases,” Brazelton says. But lax oversight and corruption during recent decades of breakneck economic growth has led to a string of product quality scandals in China — from baby formula cut with industrial chemicals to contaminated blood thinner and tainted vaccines.”
Now, as the government rushes to try and vaccinate more people, they seem to be pulling out every stop short of using foreign mRNA vaccines, seemingly sticking to the most flawed gun in the safe. Furthermore, this points to a complicated and sensitive situation for Chinese citizens as they try to balance the realities of heavily censored channels of communication, poor signaling and a history of mismanagement from the government, and a desire to protect themselves as best as possible. This situation, unfortunately, is likely to get much worse in the coming weeks as the healthcare system is overwhelmed.
Growing Danger for China’s Broken Healthcare System
Much of the world watched in horror in February 2020 as time lapse footage of Wuhan’s nearly overnight construction of two temporary hospitals to manage COVID-19 cases as the city’s normal hospitals became overburdened dominated news coverage. This wasn’t unique in the government’s epidemic playbook, as it had similarly erected the Xiaotangshan Hospital in Beijing amid the outbreak of SARS in 2003. However, it highlights an important flaw in the playbook. This kind of construction doesn’t really do much in the absence of an appropriately sized and prepared healthcare workforce. China faced a shortage of physicians and nurses well before the pandemic, a fact made much worse once case counts soared in 2020. Furthermore, as diseases spread across the country, Chinese rural citizens are typically left much less protected than their urban counterparts. These are central issues to the looming COVID-19 crisis unfurling in the country today.
The PRC has undergone significant healthcare reforms in the last decade or so, in large part through the Healthy China 2020 initiative, which sought to cut healthcare costs by increasing the percentage of care covered by insurance. Furthermore, as of 2020, about 95% of the population has at least some form of health insurance, though it typically covers only about half of medical costs. Coverage is split between employee medical insurance for employed urban residents, and resident medical insurance for unemployed urban and rural residents. About 75% of those insured in the country are insured by the resident medical insurance program, pointing to the sheer portion of the population that is either rural and unemployed.
This is an especially concerning fact as the healthcare system is overly reliant on urban hospitals for basic healthcare. The United States-China Economic and Security Review Commission (USCC) notes that hospitals account for 3.5% of medical institutions in China despite handling 45% of all outpatient visits. So, while the Party views quality healthcare delivery as an important part of its political agenda and there have been improvements in coverage and care, there are still serious issues in providing quality care nationally. As is often the case, corruption is a large part of this problem. As the USCC explains:
“Corruption among China’s hospitals and doctors is a widely acknowledged problem that has contributed to a low level of public trust in the country’s healthcare system and at times led to violence against Chinese doctors. In many cases, doctors accept illicit payments, known as hongbao, from patients in exchange for a higher quality of care. The practice of hongbao is widespread in China: in a 2013 survey of residents of Beijing, Shanghai, and Guangzhou, nearly one-third of respondents said they or a family member had given hongbao to physicians between 2000 and 2012. In addition to accepting these payments from patients, doctors and hospital officials also receive kickbacks for purchasing certain types of medical equipment or pharmaceutical products, a practice that has been described as “endemic” in China. In a 2010 survey of Chinese doctors, 78 percent of respondents said healthcare companies could not compete in China without paying bribes.”
This seems to bleed into patient distrust of medical clinics, interestingly, contributing to the over-reliance on hospitals to treat minor conditions. Beyond simple perceived incompetence of clinic physicians, there is a cycle of patient-physician mistrust at this level, as Nie at al. have discussed in Developing World Bioethics. They write, “Mistrust (particularly physicians’ distrust of patients and their relatives) leads to increased levels of fear and self-protection by doctors which exacerbate difficulties in communication; in turn, this increases physician workloads, adding to a strong sense of injustice and victimization. These factors produce poorer healthcare outcomes and increasingly discontented and angry patients, escalate conflicts and disputes, and result in negative media coverage, all these ultimately contributing to even greater levels of mistrust.”
This is worse at small clinics, with providers enduring verbal and physical abuse at the hands of patients’ loved ones. There is even a recently coined term, zhiye yilao that describes a “medical mob”, or “people who support families and their relatives in demanding financial compensation from hospitals following medical disputes, as Nie et al. highlight. While many of China’s elites can afford to simply seek care at a private hospital, this is not the case for the majority of Chinese who rely on public hospitals and clinics for their care, particularly those who live in rural areas.
Rural citizens typically either use small clinics or travel to wait in lines in an attempt to get into a hospital, further burdening the system. These rural clinics are often understaffed and poorly equipped, and the national health insurance scheme creates incentives to hospitalize people with relatively minor problems, which is especially problematic for these rural populations. Socioeconomic determinants associated with rural living and resources also contribute to the stark difference in health outcomes between China’s urban and rural populations. Rural residents also are at higher risk of developing many chronic conditions like heart disease, putting them at increased risk during outbreaks of infectious diseases like COVID-19.
As cases climb in urban centers, there are distressing signs that the much better-equipped urban hospitals are becoming overrun. As we discussed, many hospitals are requiring sick staff to still come into work as individual patient loads continue to swell. We and others have also stressed, too, that China does not have the kind of ICU capacity needed to deal with what it faces. This is true in urban centers, but even more so in rural areas, where there are also 30% fewer healthcare workers available. Furthermore, retired physicians and other professionals across the country are currently being called upon to help support efforts to combat the current surge in Beijing. All these signs point to major trouble in urban centers, indicating it is likely to be much worse for rural regions of the country.
As the Spring Festival travel rush, chunyun, approaches, many will travel from urban centers to their rural hometowns, likely spreading COVID-19 to these vulnerable areas. While many are currently opting to stay home on their own and a number of universities have given students the option to finish the semester virtually to cut down on travel, these factors might not be enough to protect these places from becoming overwhelmed in the coming weeks. As a result, the Party has urged local governments to upgrade their facilities and prepare for the oncoming waves. South China Morning Postreports that, “In a directive on Sunday, the Joint Prevention and Control Mechanism of the State Council asked rural hospitals and clinics to ensure pandemic medical services and timely treatment for high-risk patients, such as the elderly and people with underlying diseases.”
The directive reads in part, “Rural areas should…improve the ability of county-level hospitals to treat severe cases, and give full play to the role of health monitoring in township hospitals and village clinics to minimise the severity rate and mortality rate.” However, there is clearly no overnight fix for the kinds of deficiencies rural healthcare facilities struggle with. Despite this, Ma Xiaowei, Director of the National Health Commission, demanded on Wednesday that hospitals address swamped emergency rooms and get patients admitted to different departments. Ma also requested that medium and large hospitals accept more severe cases while promising that regulators will not hold them accountable for increasing fatality rates, according to the Financial Times.
Imploring under-equipped rural healthcare institutions and swamped urbans ones to suddenly improve their ability to treat an onslaught of severe cases is almost an unimaginable request, even for the State Council, as the country had over two years to get ready for its Zero-COVID exit. This complete failure of policymaking and pandemic management will almost certainly cost an unimaginable number of lives, irreversibly harm many people who do survive, further damage China’s and the global economy, and leave many demanding to know why the government did not prepare for this during the years the country spent shutdown.
What Does All This Mean Long-Term?
Just a couple weeks ago, testing positive for COVID-19, even if symptoms were mild or non-existent, was an express ticket to a government quarantine center for however long it took until the government decided one could leave. Shanghai shutdown for all of April and May just months ago, wreaking havoc on the local and national economy and causing global supply chain disruptions. The Party spent the last couple years pushing the message that this “devil” virus was so incredibly dangerous that it was worth it to continue these lockdowns and economic hardships. Today, however, the government insists COVID-19 is basically a cold, that nothing much will come of being infected, and that everything from herbal supplements to canned peaches are good remedies for it. This complete turnaround has many anxiously waiting for the economic consequences and wondering what this means for Xi Jinping and the Party in the long-run.
It’s the Economy, Shagua!
The CCP and State Council recently wrapped up the annual Central Economic Work Conference (CEWC), a meeting that sets the Party’s national economic agenda and directives for the financial and banking sector for the next year. At the meeting, Xi Jinping, who has been remarkably quiet since the end of Zero-COVID, gave a speech in which he indicated that China’s economy is expected to recover and improve in 2023, a tall order given the situation. A number of other critical points were made in an attempt to address the intense downward pressure the national economy is under, explicitly recognizing that the domestic economy has weak prospects coupled with unstable supply chains and shrinking demand.
Another critical point of the CEWC was that, “The meeting urged efforts to deepen the reform of state-owned enterprises (SOEs) while improving their core competitiveness, requiring that legal and institutional arrangements must be made to ensure the equal treatment of private enterprises and SOEs.” While China’s 2001 accession into the World trade Organization was contingent on achieving predominantly “market economy conditions,” the Chinese economy never truly transformed into a market-based one. Rather, despite some reforms in the 1990s and early 2000s, the government has maintained large SOEs in strategic and financial sectors while also maintaining policies that strongly favor these companies. Nicholas Borst explained the logic behind this succinctly for the Lowy Institute, writing “Rather than allowing the private sector more space, Beijing wants a tool for the implementation of government policy.”
In 2021, China had over 150,000 SOEs, with most of its FortuneGlobal 500 companies under state control. In 2019, SOEs accounted for more than 60% of the PRC’s market capitalization while accounting for 40% of its national GDP. For context, in 2019, Chinese SOEs made up more than 4.5% of the global economy–and now they are going to be treated equally with private businesses in China. This marks an important change as the Party also looks to increase demand by ensuring higher quality supply, and get a better hold on the deleveraging of the country’s real estate industry, stating that bail outs will come only if companies have well-founded plans for recovery. Just last month, amid further reduced apartment sales, the cabinet urged banks (again, most of which are SOEs) to increase loans for completion of unfinished apartments, with the central People’s Bank of China going so far as to reduce “by $70 billion the money that the country’s commercial banks are together required to hold for emergencies, freeing them to lend that money instead.”
Is This China’s Lehman Moment?
The current real estate crisis in China offers a particularly concerning look into just how damaging the sudden removal of Zero-COVID policies in the country could be both domestically and internationally. In recent years, it has been clear China’s real estate market was heading for trouble, with many people paying mortgages on apartments that are not even finished contrasting with the estimated 65 million units (1/5 of the homes available in the country) sitting completely open in China’s ghost cities. In late September last year, China Evergrande Group, China’s second largest property group, was forced to begin payments on its hundreds of billions of dollars in debt amid new regulations on developers’ debt limits. This started the current real estate sector crisis as when it caused several stock market indices to drop on September 20, 2021.
In the last year, it seemed that the Party was concerned the crisis would worsen in the absence of Zero-COVID restrictions. As Keith Bradsher explains in the New York Times, “Real estate development plays an outsize role in China’s economy, representing about a quarter of economic output and a quarter of its bank loans. Housing represents at least three-fifths of household assets in China, and many Chinese regard apartments as the only reliable way to build wealth.” This seemed to leave the Party locked into the restrictions in an effort to protect such an important but struggling part of its economy. Today, however, Zero-COVID is dead and the Party has indicated it wants less borrowing overall and that companies will only be bailed out if they present “well-founded” plans.
In the last year, the government has spent heavily on new railways and other infrastructure investments to try and help the economy amid low confidence, but that was with consistent COVID-19 policies in place. Furthermore, there have been concerns that injecting too much credit too quickly would be counterproductive to the goals of getting companies to borrow less and strengthen their balance sheets. In the real estate sector, the country has to somehow balance achieving sustainable growth and lowering prices, but that is not going to happen if sales keep falling. For example, in Shanghai this year, luxury apartment prices fell as much as 40% after the Party Congress because of concerns about the economic and political direction the country will take in Xi Jinping’s third term.
The CCP is Anything but a Party Right Now
Today, it is hard to fault those in Shanghai for selling off their multi-million dollar properties while they could. Models range in their estimated COVID-19 deaths in China in the absence of Zero-COVID, with some predicting under one million and some going over two million. This high of a number of deaths so suddenly, particularly as a result of the sudden end of virtually all precautions after years of constant testing and lockdowns, will be politically difficult to manage.
This also does not touch on how many Chinese will likely suffer from Long COVID and other long-term conditions if they do recover from COVID-19, something many other countries have had to learn the hard way. In the US, it is estimated that Long COVID costs the economy $3.7 trillion. While the US certainly has struggled with its COVID-19 response, it at least has effective vaccines. In September, Chinese state media was full of pieces talking about the “West’s hidden pandemic” of Long COVID and, now, it is nearly impossible to find any PRC official discussing this condition. The narrative has done a complete 180° on all fronts.
The threat of suddenly losing one million people completely and leaving an untold number burdened with long-lasting symptoms should be enough to make anyone reconsider their policy decisions. However, this is difficult for someone like Xi Jinping who has spent years building an image of infallibility while also championing Zero-COVID the last two years. He has often relied on rhetoric describing pandemic response as a war and continuously touted China’s unique approach as a better alternative to the “chaos of the West.” It is hard to believe what is happening in Xi’s China today is anything but complete chaos, and no amount of internet censorship and state media pieces about the supposed correctness of this new approach can keep the population totally unaware of that fact.
It still is not clear why Xi Jinping suddenly reversed course on Zero-COVID, even in the face of protests against the largely unpopular policy. Furthermore, as Xi begins his historic third term, he does so coming off a year of remarkable failure. As James Palmer recently pointed out in Foreign Policy, the once seemingly boring, safe choice in Chinese politics has proven to be anything but in the years since he took power, eliminated competition, and doubled down on state control over every facet of life in his country. Now, with mass death and further economic turmoil on the horizon, what will happen next for Xi Jinping and the CCP?
Dr. Hassell began the event by highlighting the misconceptions associated with the terms “convergence” and “bioconvergence” within the field. His concern was that these terms have become buzzwords within biodefense and their use implies that the different fields and disciplines necessary for biodefense are converging or cooperating organically. Such a misconception leads those within and outside of the field to assume that unity of effort is common and effortless, which is not the case. Barriers to convergence are prevalent and numerous, both in government and private sectors. Dr. Hassell provided an example from his previous experience in the Department of Defense developing chemical detectors, comparing a lack of higher-level convergence to the lack of standardized interfaces on different detectors preventing operators from gaining competency on all systems after mastering any single system. Such stove-piping of systems and efforts prevents convergence and is common across biodefense. The solution is a greater degree of crosstalk between disciplines working towards a unified solution or goal. Providing another example of this failure of convergence, Dr. Hassell highlighted the recent Pentagon appropriations for biodefense failing to account for the need for cyber funding to be successful against future threats as that discipline becomes more critical.
Dr. Hassell also indicated that biological threats, in addition to the biodefense, are converging. As biotechnology and other life sciences continue to advance, the line between chemical and biological threats blurs. Previous research has demonstrated this growing convergence, from opioid-producing yeast conducted by Galanie et al. published in Nature to chemical synthesis of toxins conducted by Matinkhoo et al. in the Journal of the American Chemical Society. He urges a greater convergence of chemical and biodefense disciplines to effectively overcome these threats in the future. Such efforts would come at a substantial cost and require the reorganization of numerous government agencies, but it may be necessary to respond to the evolving threat landscape and enable more efficient use of future funding to unify efforts.
Dr. Hassell then commented on the need for greater inclusion of data sciences, data technologies, and nanotechnologies in future biodefense efforts. The necessity of greater convergence between chemical and biodefense and the inclusion of these disciplines is a key requirement identified in Biodefense in the Age of Synthetic Biology, a report prepared by the National Academies for the Department of Defense in 2018. The addition of these technology-based disciplines is indicative of a greater requirement for technology convergence in chemical and biodefense efforts to combat the rising technology integration in the threat landscape. Modern biotechnology has created significant risk of dual use to create ever greater biological threats. Dr. Hassell pointed to the recent “Dual Use of Artificial-Intelligence-Powered Drug Discovery,” published by Urbina et al. in Nature Machine Learning, that indicated how easy it may be for a machine learning system designed with the best of intentions to identify new therapeutic disease inhibitors to be reprogrammed to instead identify novel toxin molecules. In that report, the MegaSyn system was able to generate 40,000 novel VX molecules in less than 6 hours. Dr. Sonia Ben Ouagrham-Gormley, Associate Professor at George Mason University and author of Barriers to Bioweapons, indicated such results do not directly equate to actionable threats on the Radiolab episode 40,000 Recipes for Murder that covered this journal article, but they still are indicative of the evolving chemical and biological threat landscape. Dr. Hassell also indicated the convergence of other disciplines critical to future biological threats, including climate change, which is enabling greater zoonotic spillover events, generating new and often novel biological threats.
Dr. Pardis Sabeti underscored deadly infectious diseases as an existential threat to humanity during her remarks. She agreed with Dr. Hassell’s call for greater convergence and stated we must aspire to use technology to outpace the evolution of diseases so that we can be more anticipatory and less reactionary in the face of future outbreaks. She emphasized that COVID-19, though a recent a traumatic pandemic, is not the biggest threat we have faced or could face in the future. She argued we are on the precipice of cataclysm if we do not relentlessly pursue these efforts of convergence to enhance biodefense. Infectious disease is an existential threat that we can address because the tools necessary for biodefense are not bespoke or esoteric. Effective current and future biodefense tools, she argued, must be broad spectrum, offer daily value, contain transferrable benefits and knowledge, and be embraced at a cultural level to be effective. In line with the previous CSR webinar on COVID-19, Dr. Sabeti called for a greater commitment to community engagement as a key effort to combat future biological threats.
Dr. Akhila Kosaraju then emphasized the need to take novel technologies required for biodefense out of the lab and into the field. She also supported the need for greater convergence, stating such efforts must be intentional to be successful. Her company, Phare Bio, exemplifies such efforts, employing AI and deep learning to enable rapid antibiotic discovery to overcome rising drug resistances. This approach provides Phare Bio a strategy to overcome the drug development “valley of death” where most current pharmaceutical development fails and presents an opportunity for other organizations like it across biodefense. Modern biodefense efforts must emphasize biotechnology, relying on computational biologists, bioengineers, and other technical experts to maximize advances in the field. She also indicated a need for organizations like The Audacious Project, a backer of Phare Bio, to effectively unify disciplines to solve intractable problems like drug resistance. The Audacious Project is a “collaborative funding initiative catalyzing social impact on a grand scale” across a broad range of disciplines that seeks to de-risk and encourage innovation. Injection of philanthropic, grant, or even government funding sources to adequately de-risk the “valley of death” and other obstacles is essential to future preventative and treatment therapeutics. Additionally, biodefense must strive to recognize small players in the field that often offer bespoke technologies and solutions that can accelerate efforts beyond that of the usual bigger players, as demonstrated throughout the COVID-19 pandemic. Efforts like Operation Warp Speed serve as foundational examples to the benefits such efforts can provide to the future of biodefense.
This message was emphasized throughout the event, refocusing attention from COVID-19 to all pandemic response, and mirroring the call for greater broad-spectrum protection in biodefense as made by Dr. Gregory Koblentz in his book Living Weapons. Such efforts, according to Dr. Koblentz, transcend the historical “one bug, one drug” paradigm and provide a biodefense countermeasure strategy for both biological weapons and natural diseases. Broad-spectrum efforts such as these have already demonstrated their value in the response to other threats, including the adaption of existing mRNA vaccines for COVID-19 or the JYNNEOS smallpox vaccine for the ongoing monkeypox outbreak, and could prove critical in the event of any future disease outbreak or biological attack.
Dr. Hepburn opened the event with a call to action, stating all the progress we have made is good, but we still have much more work to do. He pointed to the first section of the Annual Report as a reminder of all the government has accomplished in pandemic preparedness. When asked by Ms.Wu if he believed we had learned enough from COVID-19 to prevent the next outbreak from reaching the same level, Dr. Hepburn emphatically replied “Yes.” He cautioned that the hard part is learning the right lessons and making the changes necessary to prepare. Dr. Cox stated she hoped he was right, but we also thought we were prepared for COVID-19.
Speaking on the importance of a diversified public health workforce, Dr. Hepburn highlighted the need for technologically savvy professionals. He asserted future public health workers must be trained in data analysis, program management, and human empathy to be successful. Dr. Cox then stressed the benefit of fellowship opportunities to provide professionals in the field a broader perspective to address biological threats that enhance disease outbreak prevention.
A diverse workforce is not the only ingredient needed for preparedness success. Dr. Hepburn and Dr. Cox also discussed the essential nature of interagency and private sector cooperation to overcome COVID-19 and future pandemics. This message aligns with both the 2018 National Biodefense Strategy Goal 1 and the 2021 Biodefense Vision Memo that call for greater coordination and unity of effort across all biodefense organizations in response to natural and man-made pathogens. This message is also supported by the broad range of organizations and their accomplishments throughout COVID-19 response outlined in the first section of the Annual Report. Such unity and diversity of effort is critical to maximize biodefense; including biosurveillance efforts like that of the Center for Forecasting and Outbreak Analytics, biodetection efforts from agencies like NIH RADx, and preparedness guidance from agencies like ASPR. Such multifaceted preparedness and response are essential to provide broad-spectrum protections against future threats.
A specific topic of discussion during the event was efforts in rapid production of medical countermeasures (MCM). Operation Warp Speed demonstrated we now possess the capability to produce effective vaccines within a year, enabling us to respond rapidly to emerging threats. Dr. Shulkin provides a concise summary of the essential lessons learned by Operation Warp Speed that should be applied to future vaccine development in his commentary, “What Health Care Can Learn from Operation Warp Speed.” The speakers emphasized that such efforts must become routine and require global cooperation to be effective in facing current pathogens like malaria as well as future threats. The development of vaccines is a balancing act of cost and innovation which may require government agencies to de-risk programs to incentivize innovation when the cost prohibits private sector interest. They also discussed the importance of novel vaccines that offer shelf-stable solutions as well as varied delivery methods (microneedle, oral, skin patches) to enhance distribution capabilities and capacity. Such technologies would directly benefit defensive efforts nationally and may even enhance defensive deterrence of biological weapons based on a more robust strategic stockpile.
When asked what efforts give the panelists the greatest hope for the future, they highlighted the need to engage at the local health system and community level. Such efforts enable the establishment of trusted networks that can effectively disseminate critical health information and work to deter misinformation and disinformation. This mobilizes the population in response to threats and provides an added means of innovation that can guide future MCM and biodefense efforts. It is also critical that trust is built in advance within communities, it is not a resource you can “surge” at the time of need and COVID-19 has demonstrated the effects mistrust can have on response. Vaccine hesitancy and anti-vaccine sentiments proved to be a serious obstacle in COVID-19 response and must be addressed in a vaccine-agnostic manner to enhance current and future disease prevention and eradication.
The key messages throughout this event were consistent with those throughout the biodefense community. Interagency and international unity of effort, MCM innovation, and community involvement efforts in pandemic preparedness will enhance national biodefense. The COVID-19 pandemic is a world-changing event that may be key to reinvigorate pandemic preparedness and response efforts and, as a result, biodefense as well. As the speakers emphasized, what is critical is that the entire community applies these lessons to the whole of pandemic preparedness and response, not just COVID-19 specifically, to truly benefit from lessons learned. We cannot fail to see the forest for the trees.
The COVID-19 global pandemic has threatened public health security by adversely altering the health of patients and overwhelming hospital systems throughout the world. Not only is COVID-19 a global health threat, but antimicrobial resistance (AMR) is a public health crisis too. AMR happens when microbes become resistant to antimicrobials that are designed to kill them.[1] AMR contributes to healthcare-associated infections (HAI) in patients, which spreads within healthcare facilities and throughout the community and environment.[2] The CDC reports that “each year in the U.S., at least 2.8 million people are infected with antibiotic-resistant bacteria or fungi, and more than 35,000 people die as a result.”1 AMR is a serious public health concern, especially during the pandemic, because experts have noted that COVID-19 may have reversed the progress on reducing AMR by creating a “perfect storm” for antibiotic-resistant infections in healthcare settings.[3] How has the COVID-19 pandemic impacted AMR in clinical patients, and why is it important? This issue is important because it affects patients, who are undergoing antibiotic treatments, and healthcare systems that are trying to prevent the spread of AMR. The current literature has discussed extensively the direct and indirect effects of the COVID-19 pandemic on AMR. A group of authors focuses on the increase of secondary drug-resistant infections and how they are affecting COVID-19 patients. Another group discusses the deterioration of healthcare systems allowing AMR transmission to escalate. Other authors analyze the disruption of antibiotic stewardship and its adverse effects during the pandemic. To fight against this growing pandemic, patients should work together with their healthcare providers to learn about the troubling effects of AMR and how to prevent it from spreading by practicing enhanced antimicrobial stewardship.
Secondary Drug-Resistant Infections from AMR
The surge in AMR during the pandemic has resulted in a rise of secondary drug-resistant infections. The three drug-resistant microorganisms that will be discussed are methicillin-resistant Staphylococcus aureus (MRSA), carbapenem-resistant Enterobacterales (CREs), and Candida auris.
MRSA is commonly spread in healthcare facilities and communities, and it can cause staphylococcus infections that are usually difficult to treat because of its resistance to some antibiotics.[4] Segala et. al explain that, during the pandemic, MRSA co-infections have increased significantly in COVID-19 patients who were admitted to intensive care units (ICUs).[5] “Up to 86.4% of all COVID-19 patients admitted to the ICU received a wide spectrum antibiotic therapy,” which helps treat against a vast majority of co-infections, including MRSA.5 However, exposing patients to these unnecessary antibiotics in a combination therapy can induce AMR. In another case study completed in Italy on mechanically ventilated patients, researchers compared the proportion of ventilator associated pneumonia (VAP) due to MRSA, between COVID-19 patients and non-COVID-19 patients.5 They found VAP rates were significantly higher in COVID-19 patients due to receiving a broad spectrum antibiotic therapy. Their findings also suggest there is higher rate of MRSA colonization and environmental contamination in COVID-19 ICUs.5 MRSA has not only evolved to become more resistant to antibiotics, but it continues to spread and colonize in healthcare facilities and other communities, in addition to infecting COVID-19 patients at increasing rates.
Infographic of the Risk of CRE Infections (from CDC)
Carbapenem-Resistant Enterobacterales (CREs)
Carbapenem-resistant Enterobacterales (CREs), formerly known as CR Enterobacteriaceae and nicknamed “Nightmare bacteria,” are a large group of different types of Gram-negative bacteria, such as Escherichia coli (E. coli) and Klebsiella pneumoniae, that commonly causes multiple infections in humans and in healthcare settings. CREs also develop resistance to a group of antibiotics called carbapenems.[6]CRE infections are spread from person-to-person by infecting or colonizing people (without causing infections or symptoms), specifically contact with wounds or stool, and through medical devices that have not been properly cleaned.[7]
CREs are a threat to public health because they are difficult to treat and are resistant to almost all available antibiotics.6 Their resistance comes from producing carbapenemases, which are enzymes that spread to other germs and cause resistance in carbapenems, rendering them ineffective.4 The CDC states that high levels of antibiotic resistance in CREs necessitate more toxic and less effective treatments, harming patient outcomes.7
Studies have shown that CRE infections are increasing among COVID-19 patients. According to a recent review on CRE infections during the pandemic, “secondary infections caused by CR-Klebsiella pneumoniae (Cr-Kp) show high prevalence of co-infection in COVID-19 patients.”5 Researchers have noticed that CR-Kp colonization and infections were associated with a high mortality rate in COVID-19 patients and increased use of antimicrobial agents.5 This represents a significant challenge for both infection control and clinical practice because as new antibiotics continue to be overused, CRE infections continue to rise and manifest in healthcare facilities and throughout communities.
Candida auris on CHROMagar Candida afterSalt Sab Dulcitol Broth enrichment (from CDC)
Candida auris
Candida auris is an emerging multidrug-resistant (MDR) yeast that brings severe infections and spreads easily between hospitalized patients and nursing home residents through skin-to-skin contact.4 It can also cause invasive infections by entering the bloodstream, and even cause wound and ear infections.[8] Moreover, C. auris can trigger outbreaks in healthcare settings by contaminating hospital surfaces and medical equipment, especially if they are used for COVID-19 critical care. This indicates that patients are at high risk of C. auris colonization and infections.[9]
C.auris is an extreme public health threat to communities, and it has become a more serious concern during the pandemic. Since some patients with severe COVID-19 have required intubation and other invasive devices, they are put at a higher risk of C. auris infections; the pandemic may have contributed to an increase in these cases.[10] In another report from the CDC, 39 cases of C. auris have appeared in Florida during the pandemic that were attributed to “unconventional personal protective equipment (PPE) practices and environmental contamination.”[11] Risk factors like these have caused critically ill COVID-19 patients with C. auris infections to stay longer at ICUs and require antifungal drugs for long periods of time.5 This proves that improper and extended use of PPE has played a role in self-contamination and transmission of C. auris among COVID-19 patients.5 To prevent C. auris from spreading, especially among COVID patients, it must be detected immediately and IPC practices must be implemented.
Overall, the three different pathogens share a common goal, which is to induce AMR and increase secondary infections among patients. These drug-resistant microorganisms are a few out of the many other agents that have impacted patients during the COVID-19 pandemic.
AMR Implications for Healthcare Systems
Additionally, during the COVID-19 pandemic, the exacerbation of healthcare systems has increased transmission of AMR. Studies have shown that the rise of AMR in healthcare facilities was caused by a variety of factors, such as prolonged stays in the ICU,[12]overcrowding,[13] “contaminated PPE, increased workload among hospital staff, and prolonged glove usage.”[14] Furthermore, “shortages of PPE, staff shortages, fatigue, and deployment of inexperienced staff members with only basic training” are other factors that may contribute to the increased risk of AMR.[15] These determinants not only led to a surge in AMR, but also increases in morbidity, mortality, and healthcare costs for patients.14
To reduce AMR from escalating any further, Rawson et. al propose that social distancing, increased hand hygiene practice, and pre-emptive discharge of patients and cancellation of routine procedures are potential interventions that healthcare systems can implement during the pandemic.13 In addition, Knight et. al mention “enhanced infection prevention and PPE usage and control measures, in response to the COVID-19 pandemic, will help prevent infections and limit the spread of AMR.”15 Therefore, better health infrastructure and enhanced IPC measures set in place mean minimization of AMR amongst patients.
Disruption of Antimicrobial Stewardship
Disruption of antibiotic stewardship is another problem that needs to be addressed with the rise of AMR driven by COVID-19. Antimicrobial stewardship (AMS) is “promoting the appropriate use of antimicrobials, improving patient outcomes, reducing AMR, and decreasing spread of infections caused by multidrug-resistant organisms (MDROs).”[16] However, AMS has not been emphasized enough during the pandemic. For instance, researchers are concerned that increased antibiotic use during the pandemic could enhance the long-term threat of AMR.[17] Popescu states that “misuse and overprescribing of antibiotics, poor stewardship, and generalized lack of surveillance,” are some reasons why AMR continues to be a public health problem.[18]
Moreover, misinformation on antibiotic use (whether it is low public awareness or increased consumption of them) is another factor that may enhance the rise and spread of AMR.[19] For example, Arshad et. al explain that 44% of respondents to a population survey in Australia assumed that antibiotics could treat or prevent COVID-19, and university students in Jordan who believed in conspiracy theories around COVID-19 also thought antibiotics can cure it.[20] Additionally, clinical uncertainty about the disease process and pathology of an infection can increase antibiotic use. “When clinicians do not have all the necessary information to truly understand what is happening to the patient, they tend to prescribe more antibiotics.”17 Altogether, these factors can increase the spread of AMR and disrupt AMS.
In contrast, Toro-Alzate et. al argue that “telemedicine consultations could be useful to educate patients on improving antibiotic use.”19 But at the same time, they mention how telemedicine can also increase over-prescription of antibiotics due to physicians’ decision making.19 Because they are not with patients in-person, healthcare providers tend to misdiagnose more often and not order as much lab tests with these remote services.
#BeAntibioticsAware: Do I really need antibiotics? (from CDC)
Another AMS strategy is using social media to manage online media campaigns that combat misinformation of antibiotic use. Some organizations, such as WHO and Nigeria Centre for Disease Control, correct antimicrobial misinformation and discuss ineffectiveness of antibiotics as a treatment for COVID-19 by using their digital platforms.20 Taking everything into consideration and how the pandemic impacted the public health community, AMS must be further improved and emphasized among patients and healthcare providers to reduce AMR.
Are Hospital Stays of COVID-19Patients (with AMR) Longer than Those of Non-COVID Patients?
The literature does not yet analyze the question of whether the length of hospital stays for COVID-19 patients with AMR are longer compared to hospital stays of non-COVID-19 patients. One study has claimed that AMR has led to adverse consequences for patients, including “more prolonged hospital admissions.”[21]Srinivasan mentions and compares the patient discharge data and AMR rates between patients with influenza-like illness and COVID-19.11 Yet, the data between patients with flu and COVID-19 were collected at different time frames.
In the current literature, there is no evidence and comparison recorded between hospital stays of COVID-19 and non-COVID patients during the pandemic, over the same time period. Considering that the surge in AMR has been driven by the pandemic, and that it has caused ill patients to stay at hospitals based on their conditions, it is hypothesized that COVID-19 patients with AMR have stayed at the hospitals much longer than non-COVID patients during the pandemic. To examine this gap, further research needs to be conducted by attempting to gather data through a survey and compare hospital stay rates between COVID-19 and non-COVID patients from different hospitals in the Northern Virginia area. This would also explore the critical steps needed to treat patients with AMR and to mitigate its transmission before discharging patients.
Conclusion
Antibiotics save lives but any time antibiotics are used, they can induce side effects and lead to AMR.4 Along with the rise in AMR, COVID-19 has compounded this issue, creating more challenges for patients and hospital systems to overcome. The surge of secondary infections among patients, the exacerbation of hospital infrastructures, and the disruption of antimicrobial stewardship are the results of COVID-19’s impact on AMR.
Bibliography
Arshad, Mehreen, Syed Faisal Mahmood, Mishal Khan, and Rumina Hasan. 2020. “COVID-19, Misinformation, and Antimicrobial Resistance.” BMJ371 (November): m4501. https://doi.org/10.1136/bmj.m4501.
Centers for Disease Control and Prevention (U.S.). 2019. “Antibiotic Resistance Threats in the United States, 2019.” Centers for Disease Control and Prevention (U.S.). https://doi.org/10.15620/cdc:82532.
Chowdhary, Anuradha, and Amit Sharma. 2020. “The Lurking Scourge of Multidrug Resistant Candida Auris in Times of COVID-19 Pandemic.” Journal of Global Antimicrobial Resistance 22 (September): 175–76. https://doi.org/10.1016/j.jgar.2020.06.003.
Knight, Gwenan M., Rebecca E. Glover, McQuaid C. Finn, Ioana D. Olaru, Gallandat Karin, Quentin J. Leclerc, Naomi M. Fuller, et al. 2021. “Antimicrobial Resistance and COVID-19: Intersections and Implications.” ELife 10. http://dx.doi.org/10.7554/eLife.64139.
Majumder, Md Anwarul Azim, Sayeeda Rahman, Damian Cohall, Ambadasu Bharatha, Keerti Singh, Mainul Haque, and Marquita Gittens-St Hilaire. 2020. “Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health.” Infection and Drug Resistance 13: 4713–38. http://dx.doi.org/10.2147/IDR.S290835.
Manning, Mary Lou, Edward J. Septimus, Elizabeth S. Dodds Ashley, Sara E. Cosgrove, Mohamad G. Fakih, Steve J. Schweon, Frank E. Myers, and Julia A. Moody. 2018. “Antimicrobial Stewardship and Infection Prevention—Leveraging the Synergy: A Position Paper Update.” American Journal of Infection Control 46 (4): 364–68. https://doi.org/10.1016/j.ajic.2018.01.001.
Rawson, Timothy M, Luke S P Moore, Enrique Castro-Sanchez, Esmita Charani, Frances Davies, Giovanni Satta, Matthew J Ellington, and Alison H Holmes. 2020. “COVID-19 and the Potential Long-Term Impact on Antimicrobial Resistance.” Journal of Antimicrobial Chemotherapy 75 (7): 1681–84. https://doi.org/10.1093/jac/dkaa194.
Segala, Francesco Vladimiro, Davide Fiore Bavaro, Francesco Di Gennaro, Federica Salvati, Claudia Marotta, Annalisa Saracino, Rita Murri, and Massimo Fantoni. 2021. “Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review.” Viruses 13 (11): 2110. https://doi.org/10.3390/v13112110.
Sun Jin, Louisa and Fisher, Dale. 2021. “MDRO Transmission in Acute Hospitals during the COVID-19 Pandemic.” Wolters Kluwer Health, Inc. (34) 4: 365–371.
Toro-Alzate, Luisa, Karlijn Hofstraat, and Daniel H de Vries. 2021. “The Pandemic beyond the Pandemic: A Scoping Review on the Social Relationships between COVID-19 and Antimicrobial Resistance.” International Journal of Environmental Research and Public Health 18 (16): 1–20. https://doi.org/10.3390/ijerph18168766.
Vidyarthi, Ashima Jain, Arghya Das, and Rama Chaudhry. 2021. “Antimicrobial Resistance and COVID-19 Syndemic: Impact on Public Health.” Drug Discoveries & Therapeutics 15 (3): 124–29. https://doi.org/10.5582/ddt.2021.01052.
[4] Centers for Disease Control and Prevention (U.S.). 2019. “Antibiotic Resistance Threats in the United States, 2019.” Centers for Disease Control and Prevention (U.S.). https://doi.org/10.15620/cdc:82532.
[5] Segala, Francesco Vladimiro, Davide Fiore Bavaro, Francesco Di Gennaro, Federica Salvati, Claudia Marotta, Annalisa Saracino, Rita Murri, and Massimo Fantoni. 2021. “Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review.” Viruses 13 (11): 2110. https://doi.org/10.3390/v13112110.
[9] Chowdhary, Anuradha, and Amit Sharma. 2020. “The Lurking Scourge of Multidrug Resistant Candida Auris in Times of COVID-19 Pandemic.” Journal of Global Antimicrobial Resistance 22 (September): 175–76. https://doi.org/10.1016/j.jgar.2020.06.003.
[12] Vidyarthi, Ashima Jain, Arghya Das, and Rama Chaudhry. 2021. “Antimicrobial Resistance and COVID-19 Syndemic: Impact on Public Health.” Drug Discoveries & Therapeutics 15 (3): 124–29. https://doi.org/10.5582/ddt.2021.01052.
[13] Rawson, Timothy M, Luke S P Moore, Enrique Castro-Sanchez, Esmita Charani, Frances Davies, Giovanni Satta, Matthew J Ellington, and Alison H Holmes. 2020. “COVID-19 and the Potential Long-Term Impact on Antimicrobial Resistance.” Journal of Antimicrobial Chemotherapy 75 (7): 1681–84. https://doi.org/10.1093/jac/dkaa194.
[14] Sun Jin, Louisa and Fisher, Dale. 2021. “MDRO Transmission in Acute Hospitals during the COVID-19 Pandemic.” Wolters Kluwer Health, Inc. (34) 4: 365–371.
[15] Knight, Gwenan M., Rebecca E. Glover, McQuaid C. Finn, Ioana D. Olaru, Gallandat Karin, Quentin J. Leclerc, Naomi M. Fuller, et al. 2021. “Antimicrobial Resistance and COVID-19: Intersections and Implications.” ELife 10. http://dx.doi.org/10.7554/eLife.64139.
[16] Manning, Mary Lou, Edward J. Septimus, Elizabeth S. Dodds Ashley, Sara E. Cosgrove, Mohamad G. Fakih, Steve J. Schweon, Frank E. Myers, and Julia A. Moody. 2018. “Antimicrobial Stewardship and Infection Prevention—Leveraging the Synergy: A Position Paper Update.” American Journal of Infection Control 46 (4): 364–68. https://doi.org/10.1016/j.ajic.2018.01.001.
[19] Toro-Alzate, Luisa, Karlijn Hofstraat, and Daniel H de Vries. 2021. “The Pandemic beyond the Pandemic: A Scoping Review on the Social Relationships between COVID-19 and Antimicrobial Resistance.” International Journal of Environmental Research and Public Health 18 (16): 1–20. https://doi.org/10.3390/ijerph18168766.
[20] Arshad, Mehreen, Syed Faisal Mahmood, Mishal Khan, and Rumina Hasan. 2020. “COVID-19, Misinformation, and Antimicrobial Resistance.” BMJ 371 (November): m4501. https://doi.org/10.1136/bmj.m4501.
[21] Majumder, Md Anwarul Azim, Sayeeda Rahman, Damian Cohall, Ambadasu Bharatha, Keerti Singh, Mainul Haque, and Marquita Gittens-St Hilaire. 2020. “Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health.” Infection and Drug Resistance 13: 4713–38. http://dx.doi.org/10.2147/IDR.S290835.
In October of 2021, I had the privilege of attending the Medical Management of Chemical and Biological Casualties course (MCBC), offered by the U.S. Army Medical Research Institute of Chemical Defense (USAMRICD) and the U.S. Army Medical Research Institute of Infectious Disease (USAMRIID) at USAMRICD’s facility in Edgewood, MD. I learned from instructors at these two legendary institutions how to identify chemical and biological warfare (CBW) agents, diagnose the conditions they cause, and mitigate their impacts. When I applied to the Biodefense PhD program at the Schar School of Policy and Government at George Mason, I could not have predicted that during the first semester of my doctoral studies I would be cutting a classmate out of Mission Oriented Protective Posture (MOPP) gear in the Maryland woods as part of a hands-on training exercise. This course was an incredibly informative, fascinating, and fun opportunity that was an excellent supplement to my graduate education. As an aspiring scholar-practitioner, understanding how the boots-on-the-ground manage these types of events and how such an event could impact broader operations and foreign policy is invaluable.
As the course was hosted entirely at USAMRICD due to the ongoing COVID-19 pandemic, the course felt a bit more focused on chemical warfare (CW) than biological warfare (BW). However, I found this almost more enjoyable as I had virtually no understanding of CW, making this an excellent opportunity to be immersed in learning about these agents. While I understood major concepts like the supposed chemical weapons taboo and global nonproliferation efforts from my prior studies in international relations, this course offered much more in-depth, niche knowledge. For example, I learned at MCBC that mustard-lewisite (military designation HL), two chemical weapons used together, might be a desirable agent for an actor to use, depending on the target and situation in question. This is because HL has certain properties of both agents, such as a lower freeing temperature, making it better suited for both aerial spraying and ground dispersal. Understanding concepts like these are useful from an academic perspective since it provides a better understanding of how an enemy might think about using chemical weapons and how we might prioritize defensive measures in light of such threats.
Bridging the divide between academia and practice requires scholars to learn what real-world elements of their fields look like, which this course provided through its classroom and practical portions. Though this course is explicitly targeted at healthcare providers, I think the in-depth knowledge I gained about chemical and biological agent identification and attack mitigation will improve my work, which lies at the intersection of global health and defense policy. Because of this course, I now have a deeper understanding of how difficult it is to triage victims in a CBW mass casualty event and how time-consuming and complicated it would be to manage decontamination, evacuation, and treatment of victims. I now know how many autoinjectors personnel usually carry in their gas mask carrier to use for buddy aid, what types of drugs different types of military hospitals normally have supplied, and what that all means for their response capabilities in a mass casualty scenario. While the specific, little details may not be critically important to my work, having this context is extremely helpful and, hopefully, will allow me to conduct more rigorous research and make more-informed recommendations over the course of my career.
Finally, deterrence in the CBW realm is dependent on the existence of effective countermeasures and would-be attackers perceiving that their targets are able to successfully mitigate potential attacks. Having attended this training, I am confident that USAMRICD and USAMRIID are succeeding in helping strengthen that deterrent through this and other courses. While our class had about fifty people (the vast majority military personnel) in it, I constantly heard instructors stressing that this information should be taken back to attendees’ units, shared, and used to improve training back home, increasing the chances for this information to reach those responsible for responding to a chemical or biological attack. I heard numerous encouragements for officers to coordinate more closely with their units’ Chemical Corps folks or request food supply inspections from the Veterinary Corps when in doubt about food safety while deployed. It was reassuring to see instructors encouraging servicemembers to use this information proactively, particularly when so much of what our program focuses on is strong preparedness and prevention as deterrents for CBW attacks.
This course was an excellent opportunity for me to interact with professionals in fields entirely unlike my own while having fun and learning a ton. I enjoyed gaining more hands-on knowledge about CBW agents and military medicine while contemplating what this course represents in overall U.S. biodefense.
Nerve agents are very much in the news these days. Bashar al-Assad’s government in Syria repeatedly used Sarin against its own people during that country’s civil war. The Putin regime employed Novichoks in both Russia and the United Kingdom against citizens it deemed insufficiently loyal to Moscow. North Korea’s Kim Jong Un utilized VX in the assassination of his brother at an airport in Kuala Lumpur, Malaysia. Across the globe, the use of nerve agents is challenging the international nonproliferation regime in numerous ways.
Against this backdrop, Dan Kaszeta’s Toxic: A History of Nerve Agents, from Nazi Germany to Putin’s Russia provides welcome background and context on these specific types of chemical weapons. A former Chemical Officer in the US Army with decades of chemical weapons experience including multiple stints at the White House, Kaszeta offers much-needed technical expertise on the invention, production, and investigation into nerve agents. The focus specifically on nerve agents is a welcome change from many other histories that tend to lump all chemical (and sometimes biological) weapons into one amorphous “poison gas” threat with little differentiation between them. While older chemical weapons such as sulfur mustard or phosgene are sometimes mentioned in comparison with nerve agents, the author never loses his focus on his primary subject. This focus also enables Kaszeta to bypass the introduction and extensive use of chemical weapons in World War I that tends to dominate many other similar histories. Instead, Toxic begins with the Nazi discovery of Tabun, Sarin, and Soman in the context of World War II and follows the history of the dissemination of this technology to the present day.
The in-depth discussion of Nazi nerve agents is one of the real strengths of this book. Kaszeta conducted extensive archival research and revealed numerous interesting new details including insights into why nerve agents were not employed during the war, either on the battlefield or in the gas chambers. Similarly, his discussion of nerve agent development by the US, UK, and USSR during the Cold War is impressive even if it tends to focus heavily on weapon systems (likely reflecting Kaszeta’s military background). The sections on the Syrian Civil War and the Skripal poisoning in the UK are also notable for their impressive detail and valuable discussions into those investigations.
Kaszeta’s best analysis appears in recent events that he investigated as part of his work with the open-source research organization Bellingcat. He directly confronts the disinformation campaigns trying to deny Syria’s use of Sarin. The author correctly points out that much of the effort is not designed to disprove Syria’s actions, but simply muddy the waters enough to make investigators throw up their hands in defeat. Kaszeta similarly attacks Russian disinformation about the Skripal poisoning and uses a combination of technical knowledge and common-sense logic to demonstrate the weakness of Moscow’s denials. One would not expect to find much humor in a history of nerve agents, but Kaszeta’s devilish sense of humor makes several appearances, especially when disproving the lies of the Russian and Syrian governments about their nerve agent use.
That said, the book is inconsistent overall. The sections on the Aum Shinrikyo Sarin project and the VX assassination of Kim Jong Nam, in particular, lack the same level of attention as most of the others. The basics are all there, but the minimal amount of detail and the lack of insights are sometimes striking compared to other chapters. Relatedly, Kaszeta sometimes provides copious details on nerve agent production facilities and weapons systems and then fails to provide sufficient analysis of what it all means. This is nowhere more evident than in his too brief final chapter where he brings the entire history together. He, undoubtedly, has more insight to give and the book would likely be much improved if he shared more of it.
Kaszeta remains focused on nerve agents throughout his book, but he sometimes diverges from the broader historical narrative in distracting ways. The chapter on the psychological effects of nerve agents is a key example of this tendency. Kaszeta raises interesting questions about possible linkages between nerve agents and mental illness, but the topic seems out of place and his argument is underdeveloped. Perhaps lacking the appropriate medical knowledge to pursue on his own, the author simply wanted to raise the issue for others to investigate, but this story seemed a speculative diversion away from the main story.
While most of Kaszeta’s conclusions are well-reasoned, one in particular stood out as questionable. He argues correctly that nerve agents were brought into being through the ingenuity and hard work of people working for the Nazi regime and every other related discovery builds upon that breakthrough. He then makes somewhat of a leap that without this important contribution, nerve agents never would have been invented at all. This conclusion seems debatable at best. Both sides in the Cold War would have continued their chemical weapons research even without discovering the Nazi nerve agents. The science of chemistry also would have continued to advance even without the military impetus. Investigations into the organophosphate compounds that form the basis of nerve agents would have continued regardless. After all, many nerve agent discoveries were originally based on research of pesticides. While the Nazi contribution cannot be denied, the idea that nerve agents would have remained undiscovered without it seems highly unlikely.
The greatest contribution of Kaszeta’s Toxic is as a historical and technical reference on nerve agents, an important issue. The appendices, in particular, offer solid scientific descriptions of nerve agent issues and background information on several countries rarely discussed in the literature, such as the former nerve agent programs in France and Yugoslavia. Written in accessible language, the book uses Kaszeta’s scientific knowledge to shed light on important questions. For example, he argues that while Soman is more effective than either Tabun or Sarin, few countries have pursued Soman production because it involves the expensive precursor pinacolyl alcohol. He also uses this knowledge to debunk conspiracy theories. Specifically, some have argued that Sarin was only detected in Syria after a warehouse with the binary precursors of methylphosphonyl difluoride (DF) and isopropyl alcohol was bombed. As Kaszeta rightly argues, the bombing of such a building would create a massive fireball from the two flammable chemicals, which would not magically mix together to create a nerve agent. The author’s ability to apply his knowledge and experience to contemporary issues is invaluable. For anyone interested in the historical impact of chemistry or the role of chemical weapons in world affairs, this book is a worthy addition to their reading list.
The COVID-19 pandemic, which was first detected in the Chinese city of Wuhan in December 2019, has turned the world upside down. While the origins of the pandemic, either a natural spillover event from animals to humans or the result of an escaped virus from the Wuhan Institute of Virology, remain contested, there is no denying that the virus has served as a focusing event for political leaders. As a rare, sudden event that has inflicted large-scale harm upon the public, the pandemic has also functioned as a powerful catalyst for policymaking [i]. While China had been drafting new biosafety legislation since 2019, the pandemic accelerated its finalization after President Xi Jinping announced his intent to enhance biosafety measures in February 2020. The law’s approval also comes as China recently experienced one of its worst COVID flare-ups in 2021, challenging the country’s success in overcoming the virus.
On October 17, 2020, China’s Standing Committee of the 13th National People’s Congress approved the Biosafety Law of the People’s Republic of China [ii]. This law is the first of its kind, unifying numerous preexisting biosafety policies under a single framework [iii]. Yet, one may be wary of the law’s credibility in effectively addressing biosafety gaps in China’s infectious disease framework given the political drama surrounding China’s response to the pandemic. China is under heightened scrutiny as the international community questions the origin of the pandemic, China’s initial handling of the COVID-19 outbreaks in Wuhan, and whether Chinese institutions and facilities are prepared to counter future infectious disease threats. Thus, even though China proactively initiated the Biosafety Law to address biosafety concerns, its rapid completion could be seen as a reflexive action to ameliorate the international community’s skepticism. The Biosafety Law’s broad and sometimes vague approach to addressing pathogen management, biohazardous agent accountability, capacity-building, and preparedness also highlight that there is much work to be done beyond approval of the law.
China’s Biosafety Law is unlike a highly detailed US law. Rather, it is analogous to a US government-issued strategy, a high-level document setting forth broad principles for subsequent legislative actions and policies. Thus, Chinese ministries will have to subsequently provide additional details to build upon the Biosafety Law. While strategy documents retain a certain amount of ambiguity to set the stage for more prescriptive, future policies, China’s Biosafety Law exhibits a noticeable lack of clarity. An analysis of the Biosafety Law’s key elements will therefore help inform outside parties about how China plans to navigate the infectious disease and biotechnology landscape moving forward.
Prior to diving into China’s Biosafety Law, it is worth taking a few moments to describe the linguistic differences between how Western and Chinese scientific communities use the terms, biosafety and biosecurity. When using these terms, the Western scientific community references two separate, but interrelated disciplines. The Chinese scientific community commonly uses the term shengwu anquan (biosafety) while also presently developing familiarity with shengwu anbao (biosecurity). Due to the widely varying opinions on what biosecurity means depending on where one works, Chinese scientists characterize shengwu anbao (biosecurity)as a subcategory of shengwu anquan (biosafety) as opposed to an independent field of study. An unintended consequence of this is the Chinese scientific community’s tendency to use these terms interchangeably [iv]. This may be a result of China’s intent to grow their biosecurity sector under the aegis of their biosafety policies, which were made more comprehensive following the country’s 2003 SARS outbreak [v]. On the other hand, this may cause confusion to the unbeknownst reader. In an effort to best maintain the Biosafety Law’s context in this article, the evaluation below adopts China’s interpretation of biosafety and biosecurity. Therefore, readers should keep in mind that as biosecurity (as described below) encompasses the security of biotechnologies, it is applied in the context of biosafety.
China’s Biosafety Law: Why Now?
COVID-19 highlighted the absence of a central agency and legal framework in China to provide direction for policies related to the management of threats posed by infectious diseases and biotechnology. Even with nearly a hundred existing biosafety laws and regulations, China has struggled with communicating, coordinating, and enforcing biosafety regulations. This demonstrates that a variety of policies can foster inconsistencies and poor policy oversight [vi]. As a result, China’s regulations are problematically left open to interpretation by all levels of government [vii]. Left unattended, these issues could balloon into long-term complications that could disrupt or contradict efforts to combat infectious diseases. Thus, China’s new Biosafety Law is meant to unify preexisting biosafety policies under one single framework to promote national biosafety standards and regulations, and demonstrate to the world their commitment to improving biosafety practices and infectious disease preparedness.
What Does the Biosafety Law Aim to Do?
Comprised of 88 articles, China’s Biosafety Law aims to bolster prevention and response to the threat of biological agents, nurture responsible laboratory conduct, and promote stable development of biotechnology to ensure the well-being of the ecosystem and population. As a basic, all-encompassing law, it takes a broad approach to formulating supervisory parameters for various issues of concern beyond biosafety and biosecurity. It bestows the Chinese State Council—the executive body of state power in charge of carrying out policy—with the authority to enforce, oversee, and lead investigations for all activities addressed under the law [viii]. With the Biosafety Law serving as the chief blueprint, it will work towards integrating various areas to fortify national and economic security, and social stability as well as set a precedent for future policies. The main components of China’s Biosafety Law include biosafety, biosecurity, public health preparedness, ethics, and biodefense.
Biosafety Prevention and Standards
China defines biosafety as the effective prevention and response to threats of biological agents and related factors to peoples’ lives and the ecosystem, and the stable development of biotechnologies [ix]. Although the law lists various areas in which biosafety would apply, it does not clearly define laboratory safety procedures or implementation of containment principles in the event that accidental outbreaks were to take place. This is interesting as the Western definition of biosafety more clearly lists criterion and values for protecting lab personnel and the public from the threat of biological agents [x]. However, it is worth noting that biosafety is explicitly written as “an important part of national security” within the Law as numerous articles describe the boundaries of biosafety activities and appropriate behavior in China [xi]. Article 6, for example, emphasizes the need to strengthen international cooperation and fulfill biosafety obligations under international treaties. This is especially pertinent to China’s compliance to the Cartagena Protocol on Biosafety in order to improve governance over the movement of pathogens and modified organisms [xii].
Article 8 empowers individuals to report activities endangering biosafety with the goal of preventing government authorities from ignoring early warning signs and valuable information provided by experts. This is a significant provision that could provide protection for whistleblowers. During the earliest stage of the COVID-19 outbreak in Wuhan, for example, Dr. Li Wenliang, a doctor treating patients with the novel coronavirus was detained and reprimanded by Chinese authorities for raising alarms about the hazards of the virus via social media. After his death from contracting COVID-19, he was hailed as the “hero who told the truth” as the Chinese public became outraged over the initial cover-up and number of lives that could have been saved if authorities had heeded the warnings [xiii]. The inclusion of this provision should pose a sanguine outlook for whistleblower protections, but specific assurances are not described. Only time will tell how Chinese government officials will act in the future.
The biosafety-focused articles also promote joint agency collaboration to enhance biosafety capacity-building. Article 42 stipulates that China should formulate a unified biosafety standard for pathogenic microorganisms in laboratories. Article 45 establishes hierarchical management for biosafety laboratories (BSLs) to ensure that research on pathogens is carried out responsibly in appropriate BSLs as categorized by risk level. Expanding upon responsible operation of pathogens, Article 68 calls for construction of a national biosafety infrastructure to accommodate high-grade pathogens and bolster national preparedness and response. As of now, China has only two BSL-4 labs [xiv]. The Biosafety Law does not dictate which types of biocontainment labs will be built. However, China is reportedly planning on building thirty additional BSL-3 labs and at least one BSL-4 lab over the next five years [xv].
Most reflective of the COVID-19 environment is Article 70 which details the State Council’s role in ensuring “the production, supply and deployment of medical rescue equipment, treatment drugs, medical devices and other materials needed for emergency response to biosafety incidents” [xvi]. Like any other country combatting COVID-19, healthcare workers and first responders in China are on the frontlines and require proper protective gear and medical countermeasures to help those in need.
Public Health and One Health
With the pandemic sparking additional concerns about novel infectious disease outbreaks, multiple provisions of the law address public health concerns. Article 18 dictates China will establish a biosafety inventory system to catalogue important biological data, including animal and plant, and other invasive species. Article 15’s biosafety risk investigation and evaluation system, combined with Article 16’s unified national biosafety information sharing system, will then help identify animal and plant epidemic risks that endanger China’s biosafety. China is also poised to streamline communication between government departments to efficiently classify and manage potential outbreaks. Article 47 aims for more controlled management of experimental animal research in laboratories to better protect the public. These articles reflect China’s efforts to amend loopholes in its public health and biosafety systems after SARS escaped Beijing labs twice in 2004. Continued speculation of the origin of COVID-19 also places pressure upon China to straighten their public health systems.
Articles 22, 23, and 27 through 30 have a One Health focus—an interdisciplinary approach that recognizes the intersection between human, plant, and animal health [xvii]—and dedicate attention to the development of monitoring systems to trace and manage epidemics among plants and animals. Article 31 stresses the importance of strengthening capacity building measures for prevention and control of animal and plant agents at borders and ports. Article 32 expresses China’s aim to protect wildlife and prevent the spread of infectious diseases of animal origin. This will be vital for countering infectious diseases that are approximately 60-75% zoonotic [xviii]. To further champion animal and plant epidemic protections, Article 60 sets out to formulate lists of invasive alien species as guides for creating relevant management measures. By taking a One Health approach to recognizing and reducing infectious disease threats, these articles demonstrate China’s hope in preserving biodiversity, ecosystems, and the natural environment.
Security of Biotechnology Research and Applications
The Biosafety Law does not include a definition for biosecurity. Instead, biosecurity is considered a part of biotechnology dual-use research of concern (DURC). China’s singular attention to biosafety after the 2003 SARS outbreak meant that the Chinese scientific and legislative community did not become familiar with biosecurity until later on [xix]. According to Michael Barr, there are widely varying opinions on biosecurity in China and there is a “divergence of awareness” [xx] depending on where one works, but biosecurity is generally considered a subcategory of biosafety. This differs from the Western scientific community’s interpretation of biosecurity, in which biosafety and biosecurity are separate, but complementary, disciplines.
Recognizing the role of DURC in biotechnologies and how it influences pathogen management, Article 34 strengthens the safety management of biotechnology research while prohibiting research activities that endanger public health and damage ecosystems or biodiversity. Article 36 seeks to formulate biotechnology R&D standards and classifies biotechnology R&D activities as high-risk, medium-risk, and low-risk “according to the degree of risk of harm to public health, industrial agriculture, ecological environment, etc” [xxi]. Article 39 emphasizes the importance of regulating the purchase and introduction of biotechnologies and related biological factors in accordance with a control list and prohibits individuals from purchasing or possessing items on this list. The law does not provide any details on the contents of this control list.
Ethics
The Biosafety Law also covers ethical issues such as how China should improve supervision of Human Genetic Resources (HGRs). The ethical handling of HGRs has become an important issue in China after Dr. He Jiankui used CRISPR technology to produce gene-edited babies in an attempt to reduce their susceptibility to HIV [xxii]. This controversial experiment raised a number of red flags for the international scientific community—not only was it a flagrant flouting of medical and research ethics, but it also evinced China’s ineffective regulations and scientists’ lack of compliance. Therefore, Article 53 calls for strengthened supervision of the collection, preservation, and utilization of HGRs and related biological resources. Article 54, which empowers the State Council to carry out necessary investigations, provides a means of verifying compliance with these new provisions. Details on how the State Council would conduct these investigations, however, are not provided. Nonetheless, the universally negative response to Dr. He’s experiment provided a strong incentive for China to redefine its HGR regulations and reshape its bioethics standards.
Promoting Biodefense
Through Article 61 of the Biosafety Law, China hopes to “take all necessary measures to prevent biological terrorism and the threat of biological weapons”[xxiii]—echoing the Biological Weapons Convention’s (BWC) objective of prohibiting the development, manufacture, acquisition, stockpiling, possession, and utilization of biological weapons [xxiv]. China has already passed legislation for domestic implementation of the BWC and reported its biosecurity policies and enforcement measures to the United Nations Security Council’s 1540 Committee. In 2019, however, the US State Department reported that China was engaged in “biological activities with potential dual-use applications, which raises concerns regarding its compliance with the BWC” [xxv].
Article 62 tasks the State Council with creating China’s own version of the US’s Select Agent and Toxins List which is used to regulate access to dangerous pathogens that could be used by terrorists. Though criteria for this list are not described, a biological agent control list would provide China with a more formal method for managing, monitoring, and investigating suspicious purchases or activities with biological agents at risk of being misused to cause harm. Meanwhile, Article 65 calls for investigations of remnants of biological weapons found within China and the construction of facilities for their storage and disposal. The discovery and disposal of abandoned biological weapons holds historical significance for China as the country was subjected to multiple biological attacks by Japan during the Sino-Japanese War, and Chinese prisoners of war and captured civilians were victims of Japanese BW experiments conducted by Unit 731 in Manchuria during this time [xxvi]. At the end of the war, Japanese abandoned the site and destroyed records. However, recent discoveries of new records and an incubator used for the production of Yersinia pestis (the causative agent for plague) at sites in China indicates that the destruction of Unit 731’s equipment and materials was not completely thorough [xxvii]. Thus, other experimental equipment and biological munitions have the potential to be unearthed. These efforts to clean up the legacy of Japan’s biological weapons program in China complements China’s long-standing effort to safely destroy abandoned Japanese chemical weapons [xxviii].
Penalties for Violating the Biosafety Law
The Biosafety Law concludes with a final chapter on penalties for individuals who violate the law through the abuse of power, neglect of duties, engagement in malpractice for personal gain, fabrication of false information, and/or criminal acts. Penalties for such violations are financial fines that range between thousands to millions of yuan depending on the scope of the violation committed. The law does not delineate any prison time or any other form of penalties distinct from financial fines. With these current penalties, China hopes to influence scientific institutions and personnel to comply with the Biosafety Law. Yet, these articles do not describe pertinent criminal laws that would apply nor does it address whether novel criminal laws will be created to enforce the Biosafety Law—leaving the parameters for legal responsibility and investigations ambiguous.
Conclusion
Even as the Biosafety Law reflects China’s strategic positioning to incorporate biosafety, biosecurity, and biotechnology into its national security system, this ambitious set of laws needs to be accompanied by verification and accountability measures to ensure its proper implementation. What’s more, it will be interesting to see how China’s new expansive benchmarks will hold up, especially as the wording of key articles may be too broad and vague to be interpreted clearly. Nevertheless, countering infectious disease threats will be a balancing act requiring steadfast commitment and investment. COVID-19 has served as a long-awaited wake-up call for China to re-center their policy efforts and develop purposeful strategies to reduce the threats posed by natural and man-made biological threats. As the world continues to face infectious disease threats, the Biosafety Law serves as a preliminary touchstone for Chinese scientists and institutions to elaborate upon. This new law is the beginning of a long process of heightening biosafety from a local concern to a national one and developing the policies, processes, and institutions necessary to implement the law. Only then can the Biosafety Law begin to be the comprehensive and effect
[i] Thomas A. Birkland, Lessons of Disaster: Policy Change after Catastrophic Events, American Governance and Public Policy Series (Georgetown University Press, 2006), https://www.jstor.org/stable/j.ctt2tt2sn.
[iv] Michael Barr, “Cures That Kill,” China Security 4, no. 4 (2008): 33–42.
[v] Gigi Kwik Gronvall, Matthew Shearer, and Hannah Collins, National Biosafety Systems: Case studies to analyze current biosafety approaches and regulations for Brazil, China, India, Israel, Pakistan, Kenya, Russia, Singapore, the United Kingdom, and the United States (Baltimore, MD: UPMC Center for Health Security, July 2016), 8.
[ix] “Biosafety Law of the People’s Republic of China” (China National People’s Congress, October 17, 2020).
[x] Judi Sture, Simon Whitby, and Dana Perkins, “Biosafety, Biosecurity and Internationally Mandated Regulatory Regimes: Compliance Mechanisms for Education and Global Health Security,” Medicine, Conflict, and Survival 29, no. 4 (2013): 289–321, https://doi.org/10.1080/13623699.2013.841355.
[xi] “Biosafety Law of the People’s Republic of China.”
[xii] Biosafety Unit, “Parties to the Cartagena Protocol and Its Supplementary Protocol on Liability and Redress,” The Biosafety Clearing-House (BCH) (Secretariat of the Convention on Biological Diversity, March 5, 2018), https://bch.cbd.int/protocol/parties/.
[xviii] Stephanie J. Salyer et al., “Prioritizing Zoonoses for Global Health Capacity Building—Themes from One Health Zoonotic Disease Workshops in 7 Countries, 2014–2016,” Emerging Infectious Diseases 23, no. Suppl 1 (December 2017): S55–64, https://doi.org/10.3201/eid2313.170418.
[xix] Amy E Smithson, Monterey Institute of International Studies, and James Martin Center for Nonproliferation Studies, Beijing on Biohazards: Chinese Experts on Bioweapons Nonproliferation Issues (Monterey, Calif.: James Martin Center for Nonproliferation Studies (CNS). Monterey Institute of International Studies, 2007), 47, http://cns.miis.edu/reports/pdfs/beijing_on_biohazards.pdf.

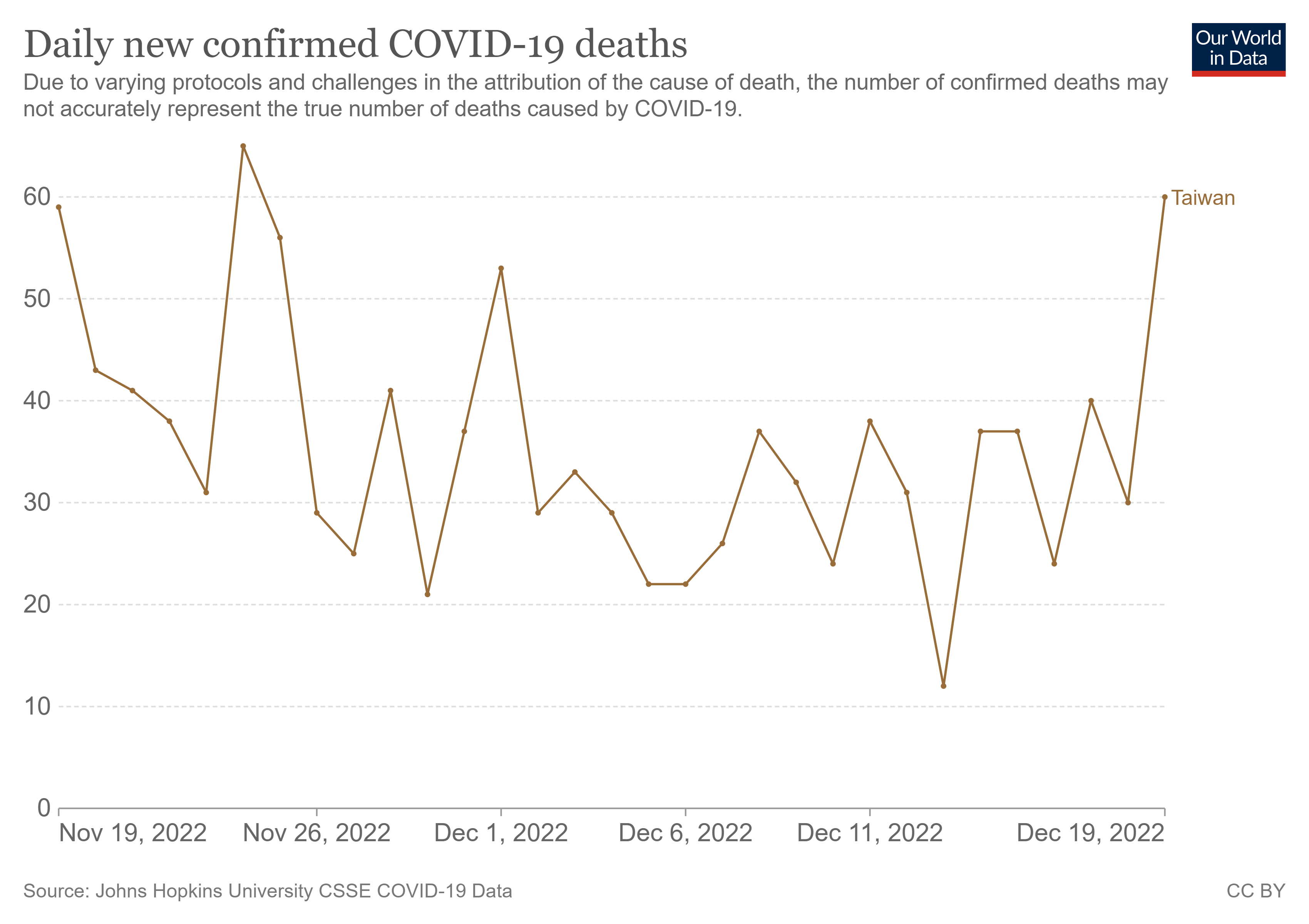
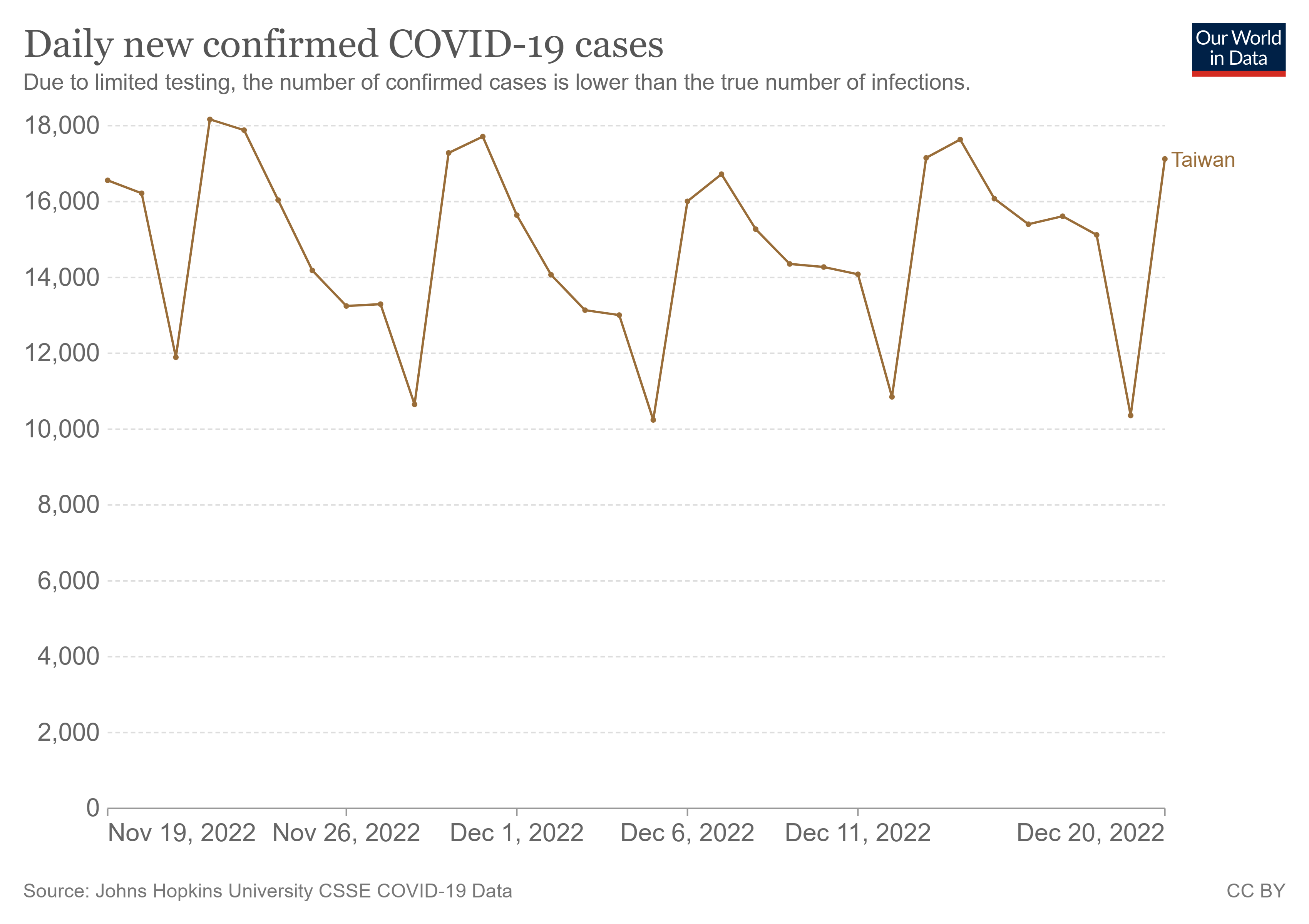

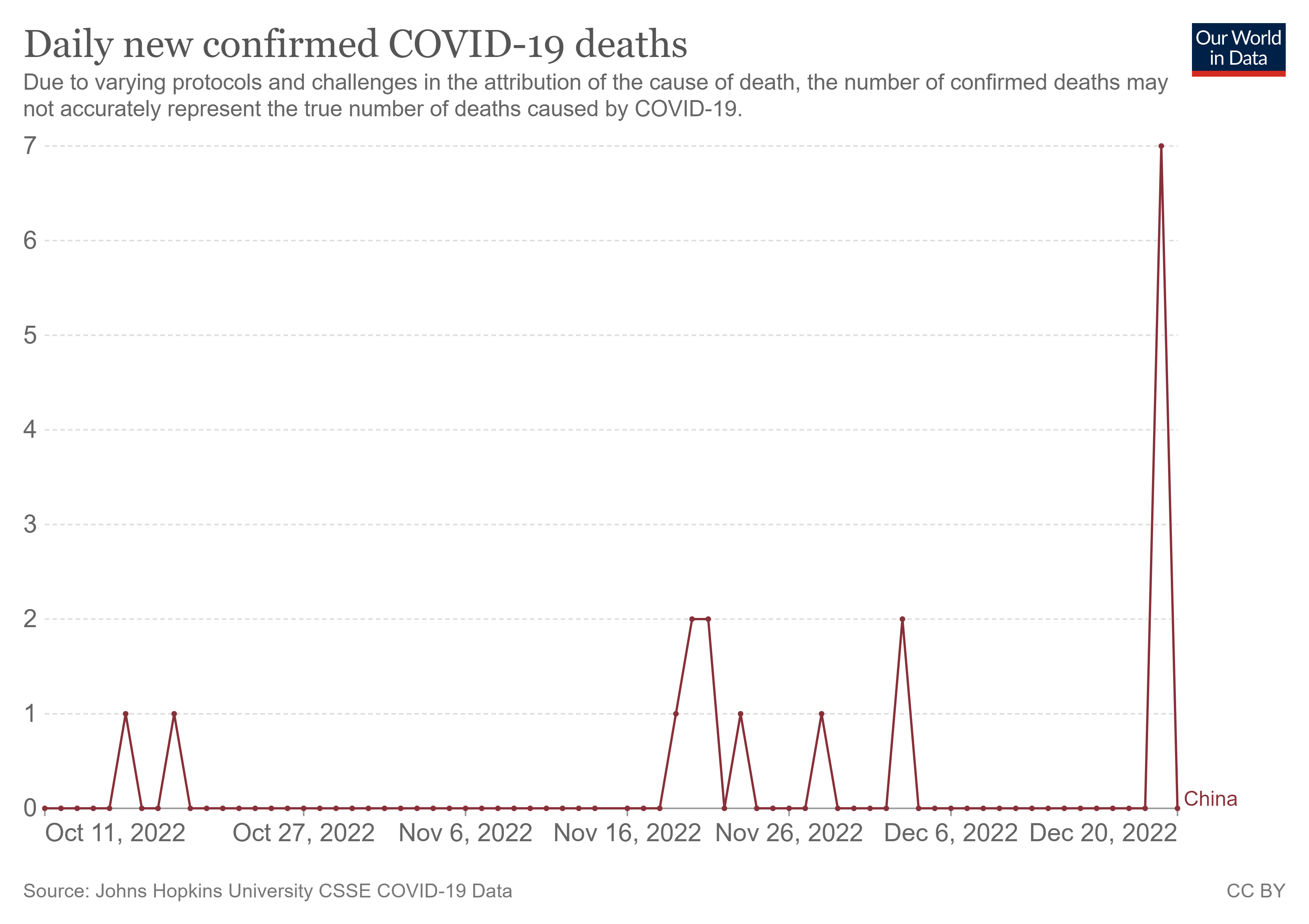
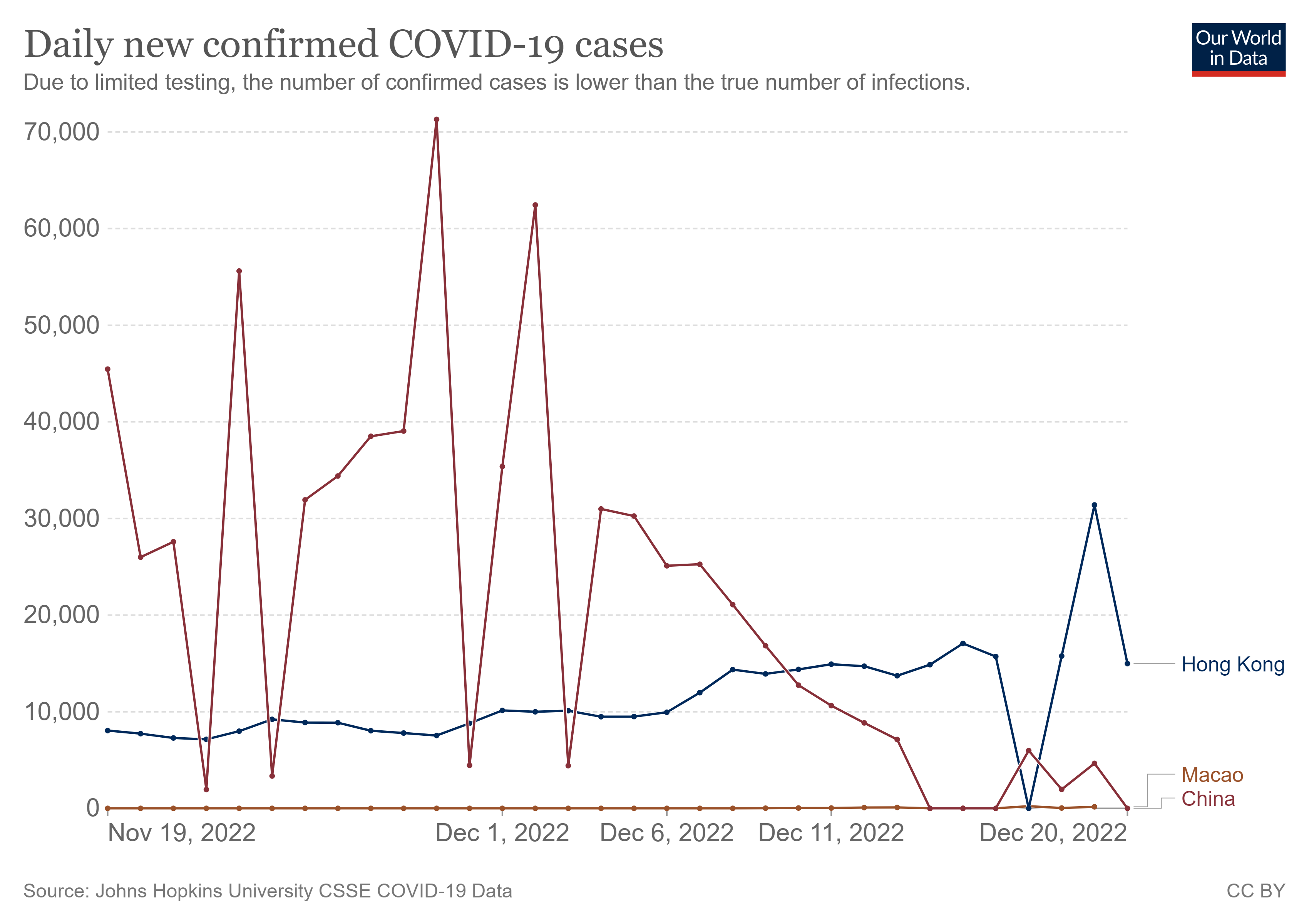
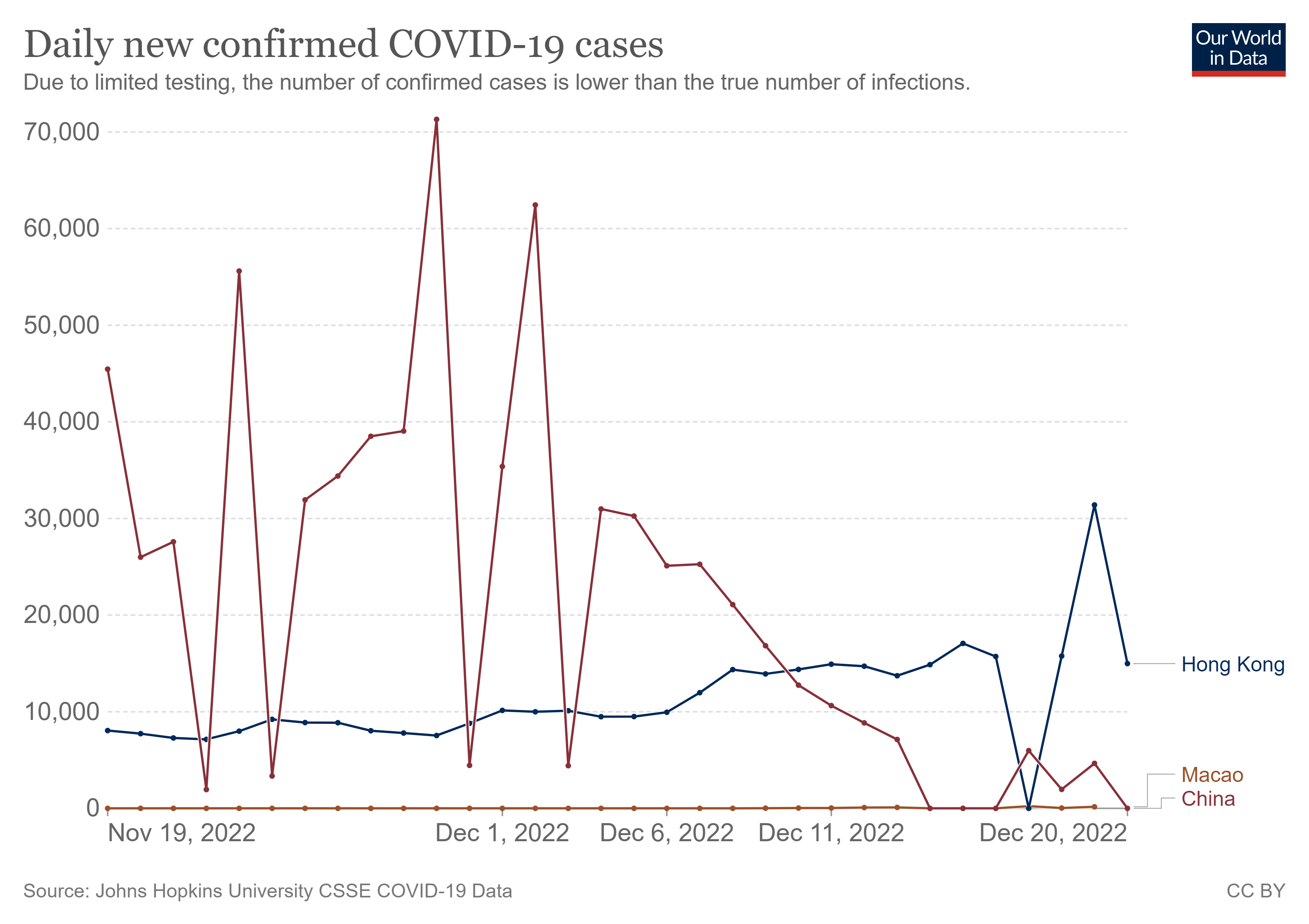

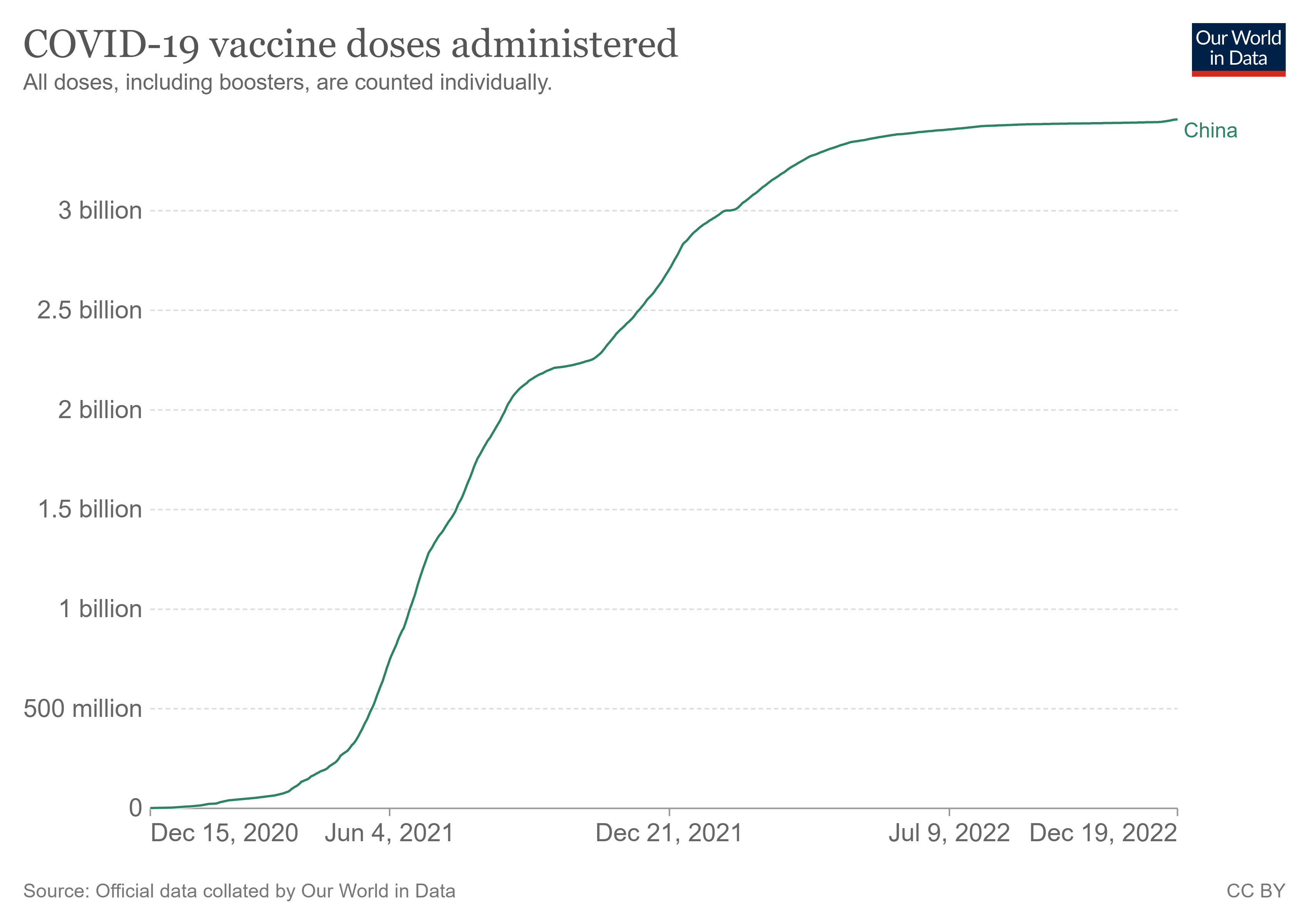
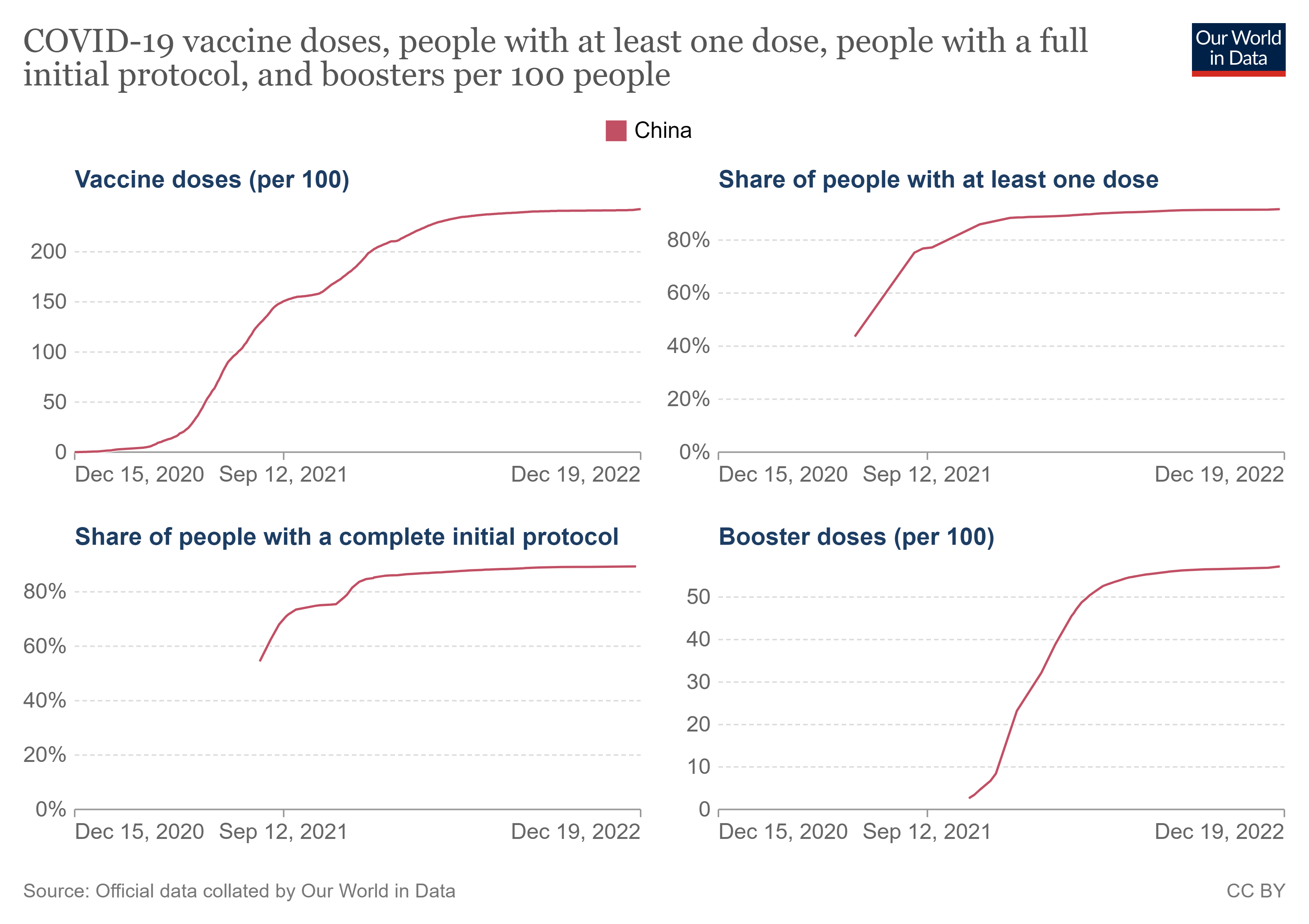








{kind=link}