
Happy almost Halloween! This week’s Pandora Report includes news from the Biodefense Graduate Program and discussion of the Biden administration’s latest National Security Memorandum, a new multilateral effort from the US, Canada, and Mexico to improve regional health security, the WHO’s praise for Rwanda’s swift and effective Marburg response, and more.
Upcoming Virtual Information Sessions on the Biodefense Graduate Program
If you are interested in a career in biodefense or global health security or want to develop the knowledge and skills necessary to work at the nexus of health, science, and security, find out what the Schar School of Policy and Government has to offer.
The Schar School PhD programs will be holding a virtual open house on Wednesday, October 30 from 6-7:30 PM. Please join Dr. Gregory Koblentz, director of the Biodefense Graduate Program, to learn more about the Biodefense PhD program and ask any questions you may have. Register here.
GMU Biodefense Students Tour Mason’s Biomedical Research Laboratory
Last week twelve Biodefense students had the opportunity to visit George Mason’s 52,000 square-foot Biomedical Research Laboratory (BRL) located on the SciTech campus in Manassas, Virginia. The BRL was inactive after being decontaminated for annual maintenance . The tour, led by the BRL’s Director of Research Operations, Rachel Pepin, provided students with a firsthand look at Mason’s Biosafety Level 3 (BSL-3) and supporting Biosafety Level 2 (BSL-2) labs. Among the many highlights was the BRL’s autoclaves and gloveboxes, which left students impressed.


The BRL is one of 12 Regional Biocontainment Labs in the United States funded by the National Institute of Allergy and Infectious Diseases NIAID. Constructed in 2010, it became an active “hot” lab in 2012. Fifteen Mason faculty members and thirty students at any time work within the facility on research pertaining to a variety of infectious diseases, new vaccines, diagnostics, and therapeutics. The stated mission of Mason’s BRL is to 1) advance pathogen biology, 2) train the future workforce to safely handle infectious agents and conduct innovative research in BSL-3 environments, 3) evaluate diagnostics, therapeutics and vaccines, and 4) serve as a resource in the event of a bioterrorism or infectious disease emergency. Overall, students gained an appreciation for the critical work and numerous safety controls in George Mason’s BSL-3 laboratory.
This write up was written by Biodefense MS Student Will MacDonald.
OPCW Workshop on Legislative and Regulatory Frameworks for Chemical Security
On October 21-22, 2024, Dr. Gregory Koblentz, director of the Biodefense Graduate Program, attended a meeting of chemical security experts sponsored by the Organization for the Prohibition of Chemical Weapons (OPCW) to discuss best practices for establishing legislative frameworks for chemical security. According to INTERPOL, from the records of 4,100 captured ISIS members, 109 of them have a background related to chemistry, science, technology, engineering, and mathematics. Meanwhile, across the word, the chemical industry and trade are rapidly growing, increasing the risk of toxic chemicals being misused, especially by non-state actors. Many countries are therefore seeking to strengthen their legal and regulatory regimes to address risks such as attacks on chemical facilities, the theft of toxic chemicals, or their release with malicious intent. Initial take-aways from the meeting included a recognition that there is an urgent need for robust national legislative frameworks for chemical security in many countries, that national threat assessments and risk analyses should be the basis for identifying legislative needs, and best practices are most useful if they can be adapted to country-specific contexts and resource setting. This meeting of an international group of chemical security experts kicks off a longer-term discussion on best practices for establishing legislative frameworks for chemical security sponsored by the Implementation Support Branch of the International Cooperation and Assistance Division at OPCW.
A Risky Review of Research
On September 25, 2024, Senator Rand Paul introduced a revised version of the Risky Research Review Act (S. 4667) which was voted out of the Senate Homeland Security and Government Affairs Committee by a vote of 8-1. In a recent OpEd in StatNews, Gregory Koblentz, director of the Biodefense Graduate Program, and David Gillum and Rebecca Moritz, past presidents of the American Biosafety Association (ABSA) wrote of the original bill: “this legislation threatens to cast a shadow over the future of life sciences research and slow it down.” While this revised bill contains some positive changes, it remains deeply flawed and does not represent a viable solution to the challenges posed by dual-use research. You can read their analysis of the good, the bad, and the ugly of the revised Risky Research Review Act here.
Russia Expanding Secret BSL-4 Lab at Sergiev Posad
The Washington Post has identified new construction activity at Sergiev Posad-6, part of the former Soviet and current Russian biological weapons program, consistent with the building of additional high containment laboratories, including BSL-4 lab suites. The construction started in 2022, shortly after Russia’s invasion of Ukraine which was accompanied by unfounded allegations that Ukraine was developing biological weapons with the help of the United States and other NATO countries. Dr. Gregory Koblentz, director of the Biodefense Graduate Program, is quoted in the article as saying, “I would not be surprised if some influential segment of the Russian national security community has drunk the Kool-Aid and really believes that the United States really is developing biological weapons.” Satellite imagery obtained and analyzed by the Washington Post has identified the construction of “10 new buildings, totaling more than 250,000 square feet, with several of them bearing hallmarks of biological labs designed to handle extremely dangerous pathogens.” The Global BioLabs Initiative identified Sergiev Posad-6 as having a BSL-4 lab in 2021. The existence of a BSL-4 lab at this site was confirmed by a 2017 scientific article co-authored by a researcher at the 48th Central Research Institute of the Ministry of Defense at Sergiev Posad. Russia has not declared the existence of a BSL-4 lab at this site on Form A of the confidence building measures that it submits to the Biological Weapons Convention.
White House Releases New National Security Memorandum on Advancing AI Leadership
The Biden administration issued this week the first-ever National Security Memorandum (MSM) on AI. The NSM direct the federal government to take steps to 1) “ensure that the United States leads the world’s development of safe, secure, and trustworthy AI,” 2) “harness cutting-edge AI technologies to advance the U.S. Government’s national security mission,” and 3) “advance international consensus and governance around AI.”
The NSM directives are focused on actions to improve chip supply chain security and diversity, making collection on competitors’ operations against the US AI sector a top-tier intelligence priority, formally designating the AI Safety Institute, doubling down on the National AI Research Resource, directing “the National Economic Council to coordinate an economic assessment of the relative competitive advantage of the United States private sector AI ecosystem,” and more.
Among its other measures, the NSM also directs the creation of a Framework to Advance AI Governance and Risk Management in National Security, which was published alongside the NSM. This framework and any successor document will specify that each covered agency has a chief AI officer and guidance boards, offer guidance on AI activities that pose “unacceptable levels of risk and that shall be prohibited,” and more.
A fact sheet for the new NSM is available here.
US, Canada, and Mexico Announce Efforts to Improve Regional Health Security
This week, the US Departments of Health and Human Services, State, Agriculture, and Homeland Security, along with their counterparts in Canada and Mexico made good on commitments made at the 2021 and 2023 North American Leaders’ Summits in releasing the North American Preparedness for Animal and Human Pandemics Initiative (NAPAHPI). NAPAHPI is “…a flexible, scalable, and cross-sectoral platform to strengthen regional capacities for prevention, preparedness, and response to a broad range of health security threats that builds on lessons learned from COVID-19 and other health security events in the last decade. It is based on a long-standing trilateral collaboration under the 2007 North American Plan for Avian and Pandemic Influenza and the 2012 North American Plan for Animal and Pandemic Influenza. This initiative recognizes that the high degree of interconnectedness among our three countries of our critical infrastructure, supply chains, and societies means that disruptions affecting one country often impact the others. Only by working together can we protect the health security of our region.”
Learn more here.
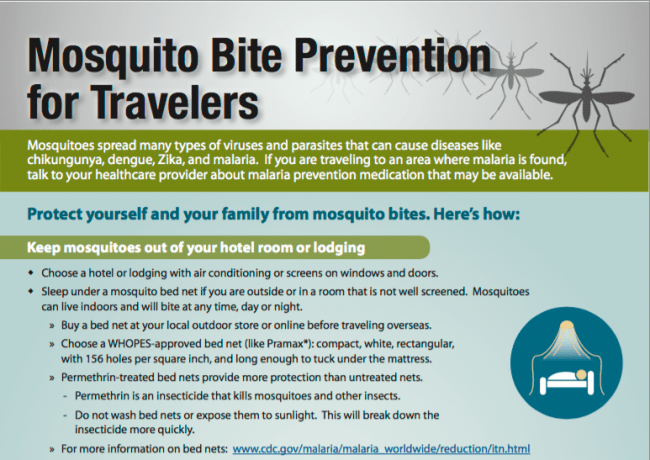
Egypt Declared Malaria Free
Egypt was officially certified malaria-free by the World Health Organization this week. Following Morocco and the UAE, Egypt is just the third country in the WHO’s Eastern Mediterranean region to receive this certification. Globally, 44 countries and one territory currently have this designation.
“This certification of Egypt as malaria-free is truly historic, and a testament to the commitment of the people and government of Egypt to rid themselves of this ancient scourge,” said WHO Director-General Tedros Adhanom Ghebreyesus in a statement. “I congratulate Egypt on this achievement, which is an inspiration to other countries in the region, and shows what’s possible with the right resources and the right tools.”
WHO Praises Rwanda’s Marburg Response
WHO Director-General Tedros Adhanom Ghebreyesus praised Rwanda’s response to its Marburg virus outbreak, noting their success in treating patients infected with this especially deadly disease. As of earlier this week, Rwanda has made it a full week with no new cases, and its total number of patients still in treatment is down to just one. “Leadership from the highest levels of government is essential in any outbreak response, and that’s what we see here in Rwanda,” Tedros said during the press briefing. The Director-General also noted that multiple patients experiencing multiple organ failure were put on life support, intubated, and eventually extubated. “We believe this is the first time patients with Marburg virus have been extubated in Africa. These patients would have died in previous outbreaks,” Tedros explained.
Burgers, Deli Meat, and Waffles-Oh My! US Responding to E. Coli and Listeria Outbreaks
It has been a rough couple of weeks for many major food suppliers in the United States amid headlines about recalls and reports of multiple cases of E. coli and listeria across the country. McDonald’s, KFC, Burger King, and other restaurant chains have pulled onions from their menus following an outbreak of E. coli traced back to McDonald’s Quarter Pounders. The CDC announced this week it is investigating 49 cases linked to “slivered onions used in the Quarter Pounder and sourced by a single supplier than serves three distribution centers.” One person is dead and ten more have been hospitalized. The supplier, Taylor Farms, has issued a recall on all of its peeled, diced, and whole peeled yellow onion packs due to potential contamination.
This comes amid multiple listeria outbreaks affecting several kinds of products, including deli meat, frozen waffles and pancakes, and even salmon. While these recalls are certainly nothing to ignore, they might not necessarily be happening more frequently than before as some have suggested. Dr. Céline Gounder, CBS News medical contributor and editor-at-large for public health at KFF Health News, told CBS this week that “Every step of food processing, there’s the opportunity for contamination. That’s number one. Consumers want ready-to-eat food, so of course, they’re more processed as a result.” She continued, saying “We have better tests. So it used to be we might not have been aware or known what made you sick. Now we can actually test, detect and tell you what made you sick.”

“Assessing the Burden of and Potential Strategies to Address Antimicrobial Resistance”
From NASEM: “Antimicrobial resistance (AMR) is linked to millions of deaths globally each year. As an evolving public health threat, there is a need to further develop methods to quantify AMR’s burden within medical practice and other sectors like food production. The National Academies Forum on Microbial Threats hosted a public workshop in March 2024 to explore the burden of AMR and discuss clinical, scientific, and policy strategies for addressing the growing AMR health threat across sectors.”
“This proceedings highlights the presentations and discussions that occurred at the workshop.”
“The Changing Face of Pandemic Risk: 2024 Report”
From GPMB: “The 21st century has seen a significant rise in global health threats. Epidemics and pandemics are now a constant danger rather than rare events. The 2024 GPMB report, The changing face of pandemic risk, is a call to action for global leaders, policy-makers, health professionals, and communities to build a safer, more resilient future. It outlines the key drivers of pandemic risk and provides a roadmap for strengthening our defences.”
“Mpox: Neglect Has Led to a More Dangerous Virus Now Spreading Across Borders, Harming and Killing People. Leaders Must Take Action to Stop Mpox Now”
McNab et al. recently published this opinion article in PLOS Global Public Health, writing in part “In other words, mpox is an ever-growing regional health crisis in Africa, and without urgent action to stop the epidemics when and where they occur, it will continue to spread across borders and continents. The few tools we have that could help to stop the outbreaks have yet to become adequately available in the most affected low-income countries where they are urgently required, as is financing to support the public health response. Mpox cannot be allowed to continue spreading widely across the African continent or anywhere. The world cannot continue to simply ‘learn’, but not apply the costly lessons of neglecting disease outbreaks.”
“Are We Ready For A Bird Flu Vaccination Campaign?”
Ram Koppaka and Richard Hughes IV discuss the possibility of H5N1 human transmission and a hypothetical mass vaccination program against this virus in this piece for Health Affairs. They write in their conclusion, “The most recent pandemic clearly demonstrated the inadequacy of our existing level of vaccine preparedness. So far, we have failed to seize this moment and put in place the infrastructure to support immunization of both children and adults. Worse still, it indicates a failure to learn some of the pandemic’s hardest lessons. As a result, we are destined to once again endure the consequences, knowing that they had been largely avoidable…Or we can do it differently this time. We can act now to be truly ready and prepared to mount a mass vaccination campaign against the next pandemic threat—whenever it comes. We have risen to the occasion before, and we can do it again.”
“COVID, Mpox, Cholera: Is the World Prepared for Another Pandemic?”
Faras Ghani discusses recent outbreaks and infectious disease developments, alongside analysis of global lack of adequate access to essential healthcare services and an interview with Dr. Ahmed Ogwell, Vice President of Global Health Strategy at the UN Foundation, in this piece for Al Jazeera.
“Inside the Bungled Bird Flu Response, Where Profits Collide With Public Health”
Katherine Eban discusses the USDA’s action or lack thereof in responding to H5N1 cases in Texas dairy cattle in this Vanity Fair article, writing in her summary “When dairy cows in Texas began falling ill with H5N1, alarmed veterinarians expected a fierce response to contain an outbreak with pandemic-sparking potential. Then politics—and, critics say, a key agency’s mandate to protect dairy-industry revenues—intervened.”
“Combining AI Breakthroughs and Better Policy to Defeat Superbugs”
Akhila Kosaraju discusses the transformative opportunity AI poses in addressing AMR in this piece for the Stanford Social Innovation Review: “Superbugs may have met their match in generative AI, but to fully tackle the crisis of antimicrobial resistance, policy makers need to find new ways to help scientists and researchers overcome long-standing obstacles and revitalize a broken antibiotic market.”
“NTI | Bio Champions Effort to Enhance Transparency to Strengthen the Biological Weapons Convention”
From NTI: “From September 30 to October 2, 2024, NTI | bio convened more than 30 experts for a workshop on enhancing transparency for bioscience research and development and bolstering confidence in compliance with the Biological Weapons Convention (BWC). Held in Amsterdam, The Netherlands, the workshop gathered an international group of participants from 15 countries spread across five continents with expertise in biosecurity and biotechnology governance and international security, as well as previous experience working to establish a verification mechanism for the BWC and involvement in ongoing discussions to strengthen the Convention.”
“The meeting updated existing concepts and generated new ideas about options to enhance transparency in regard to BWC compliance. NTI helped frame these discussions by tabling a concept paper on this topic, and the group discussed approaches to advance these goals, including through scientific and technical measures for data collection and analysis, procedural approaches, and institutional structures to house such efforts. Dozens of approaches were discussed during the meeting which will inform NTI’s continued efforts to highlight and explore promising opportunities to further advance this work.”
Read more here.
“Preparing for Ecological Disruption: A Strategic Foresight Approach to Ecological Security”
Lily Boland recently authored this report for the Council on Strategic Risks: “This report leverages insights gained from the use of strategic foresight as an approach for better anticipating how risks to global security are heightened by ecological disruption. It offers a range of use-cases for applying the foresight toolkit to the field of ecological security and to establish a knowledge base to assist practitioners, governments, and institutions in enhancing their anticipatory decision-making and planning processes for addressing the security ramifications of large-scale destabilization and decline of the biosphere and ecosystems.”
“How Zombies and Vampires Help Me Grapple with Disaster”
Neil Vora, a physician who has served in the Epidemic Intelligence Service and now treats TB patients and works with Conservation International, discusses what many in this field know all too well-an obsession with works of horror, especially those about contagions and disasters. Vora explains in part, “To help manage my anxieties about the fate of the world, I often turn to scary stories about contagions and other doomsday scenarios. This may seem counterintuitive, but I find the horror genre to be a perfect sandbox to explore pressing societal problems without real-world repercussions. Horror allows me to navigate my fears to their extremes from the comforts of my living room.”
However, the author also cautions, “But while fictionalized catastrophes help me grapple with my worst fears, I’ve also come to realize that consuming them without a critical eye can lead to a paralyzing level of despair—a luxury we can’t afford at this pivotal moment in history.”
While you’re at it, check out this episode of the Poisons and Pestilence podcast guest starring Biodefense PhD Program alumna and faculty member Saskia Popescu reviewing the films, Contagion and Outbreak, and read about her intro to the field at just 9-years-old via Richard Preston’s book, The Hot Zone.
NEW: Vision for Health Forum
From Johns Hopkins: We hope you can join us in November for the Vision for Health Forum with collaboration between Johns Hopkins Howard County Medical Center and Johns Hopkins Applied Physics Laboratory.
Panel Discussion
Moderator:
M. Shafeeq Ahmed, M.D., MBA, F.A.C.O.G
President, Johns Hopkins Howard County Medical Center
Topic: Partnership between JHHCMC and APL
Jeanette Nazarian, M.D., Vice President, Medical Affairs and Chief Medical Officer- Johns Hopkins Howard County Medical Center
Topic: Revolutionizing Health through Science and Engineering
Sheri Lewis, MPH, Deputy Mission Area Executive, Global Health -Johns Hopkins Applied Physics Lab
Topic: APL-HCMC Partnership for Project Firstline: Safeguarding Our Nation’s Frontline Healthcare Workers
Lucy Carruth, Ph.D, Assistant Program Manager- Johns Hopkins Applied Physics Lab
Brian Damit, Ph.D, Project Manager- Johns Hopkins Applied Physic Lab
This event will take place at the Johns Hopkins Applied Physics Laboratory on November 4 at 4:30 pm EST. Learn more here.
The Advancing Threat Agnostic Biodefense Webinar Series
From PNNL: “Please join us in welcoming Drs. Matthew Kasper and Lindsay Morton from the Department of Defense (DoD) Global Emerging Infections Surveillance (GEIS) program for their talk titled “Challenges and Opportunities in Pathogen Agnostic Sequencing for Public Health Surveillance: Lessons Learned From the Global Emerging Infections Surveillance Program.” This webinar will take place Tuesday, October 29th, at noon PT.”
Learn more and register here.
13th Annual Jonathan Tucker Symposium
“The James Martin Center for Nonproliferation Studies cordially invites you to the 13th annual Jonathan Tucker Symposium on chemical and biological weapons issues on November 13th and 14th, 2024.”
Among this year’s speakers are Dr. Yong-Bee Lim, an alumnus of the Biodefense PhD Program and Deputy Director of the Converging Risks Lab and Biosecurity Projects Manager at the Council on Strategic Risks, who will give a talk titled “Technology Democratization and its Implications for CBW Safety and Security: Lessons Learned from Engagement with Non-Traditional Communities.”
Learn more and register here.
One Health and the Politics of COVID-19 Book Launch
The Writer’s Center is hosting a book launch for Dr. Laura Kahn’s new book, One Health and the Politics of COVID-19 (blurb below) on November 23 at 2 pm EST in Bethesda, MD. Learn more and RSVP here.
“One Health and the Politics of COVID-19 unpacks the mysteries of COVID-19’s origins to impart important lessons for future outbreaks. The One Health concept recognizes the interconnected links among the health of humans, animals, plants, and the environment. By comparing the history, science, and clinical presentations of three different coronaviruses—SARS-CoV-1, MERS, and SARS-CoV-2 (COVID-19)—Kahn uncovers insights with important repercussions for how to prepare and avoid future pandemics. The One Health approach provides a useful framework for examining the COVID-19 pandemic. Understanding the origins of this zoonotic disease requires investigating the environmental and molecular biological factors that allowed the virus to spread to humans. The book explores the many ways in which the wild animal trade, wet markets, and the camel industry contributed to the spread of the earlier SARS-CoV-1 and MERS coronaviruses. For SARS-CoV-2 (COVID-19), Kahn examines the biosafety, biosecurity, and bioethics implications of gain-of-function research on pandemic potential pathogens. This book is a must read to understand the geopolitics of the COVID-19 pandemic.”
2024 CBD S&T Conference
From DTRA: “The CBD S&T Conference brings together the most innovative and influential chemical and biological defense community members from around the globe to share insights and collaborate on the emerging chem-bio threats of tomorrow.”
“Join the Defense Threat Reduction Agency’s (DTRA) Chemical and Biological Technologies Department in its role as the Joint Science and Technology Office (JSTO) for Chemical and Biological Defense, an integral component of the Chemical and Biological Defense Program, as we Focus Forward to uncover novel concepts and examine groundbreaking discoveries within the chem-bio defense landscape.”
“The 2024 CBD S&T Conference will be held at the Broward County Convention Center, December 2–5, 2024.”
Learn more and register here.
BID2025 Stakeholder Input Request
“From BARDA: We are excited to host our next BARDA Industry Day (BID) conference on June 30 – July 1, 2025, in Washington, D.C.! BID2025 will delve into the critical intersection of health security and sustainability with experts from various sectors to discuss cutting-edge medical countermeasure (MCM) innovations and strategies.”
“We want to make sure that the event reflects the interests of our attendees. Your feedback will help us curate sessions, speakers, and topics that are relevant and engaging for you. This short questionnaire should take no more than three minutes to complete. Please share your thoughts on what you would like to see at the conference by October 30, 2024.“
Share thoughts here.
US AI Safety Institute Issues RFI on Responsible Development of Chem-Bio Models
From AISI: “The U.S. Artificial Intelligence Safety Institute (U.S. AISI), housed within the U.S. Department of Commerce’s National Institute of Standards and Technology (NIST), released a Request for Information seeking insight from stakeholders regarding the responsible development and use of chemical and biological (chem-bio) AI models.”
“Input from a broad range of experts in this field will help the U.S. AISI to develop well-informed approaches to assess and mitigate the potential risks of chem-bio AI models, while enabling safe and responsible innovation.”
“Respondents are encouraged to provide concrete examples, best practices, case studies, and actionable recommendations where possible. The full RFI can be found here.”
“The comment period is now open and will close on December 3, 2024, at 11:59PM Eastern Time. Comments can be submitted online at www.regulations.gov, under docket no. 240920-0247.”








 Welcome to
Welcome to 





{kind=link}
{kind=link}
{kind=link}
{kind=link}