Happy Friday and welcome to our weekly rundown of all things health security!
Smallpox Could Again Be A Serious Threat
GMU Biodefense professor, graduate program director, and all around health security grand master, Dr. Gregory Koblentz, is working to make sure we’re not ignoring the threat of smallpox due to synthetic biology. The problem isn’t just within the amazing capabilities of synbio, but its dual-use nature, meaning that it has the potential to be misused by nefarious actors. This concern has become even greater with the horsepox recreated by Canadian researchers who demonstrated not only capability, but also the low cost of such work. It’s not a far jump from horsepox to smallpox, especially when we have mail-order DNA fragments available at prices that continue to lower. Koblentz notes just how much of a disaster a re-emergence of smallpox would be on a global level, especially since it’s highly contagious and routine immunization has long been gone. “If resurrecting horsepox virus provides a roadmap to synthesizing smallpox virus, then why would anyone try to synthesize it? Because there are potentially legitimate uses for. Tonix claims that the horsepox virus is a good candidate for developing a new, safer smallpox vaccine. Unfortunately, the current legal and technical safeguards against the synthesis of smallpox virus are weak and fragmented. There is no clear international legal or regulatory framework to prevent the synthesis of smallpox virus. The WHO has a policy banning the synthesis of the smallpox and regulating who can produce and possess large fragments of smallpox DNA, but it hasn’t been widely adopted by states. Furthermore, there is no mechanism—at either the national or international level—for detecting or punishing violations of this policy.” Aside from some substantial gaps in regulations, there are some voluntary industry screening processes however, these are pretty limited and tend to be minimal at best. Koblentz points out that there is still time to get ahead of the pox in this case – specifically by rallying international organizations, national governments, the DNA synthesis industry, and the synbio community. Check out his recommendations and comments in the article here!
Global Health Security Supplement – CDC’s EID Journal
Don’t miss out on this ahead-of-print alert for the December edition of the CDC’s Emerging Infectious Disease journal. Volume 23 will include a section on global health security, with articles on the contributions made by the CDC and other partners, establishment of the CDC Global Rapid Response Team, and Joint External Evaluations. There’s also a great commentary by Dr. Michael T. Osterholm on the unfinished journey of global health security. “All countries need to have the laboratory, trained workforce, surveillance, and emergency operations capabilities to prevent, detect, and respond to disease threats. Only when these accomplishments are realized can we truly be on the road to global health security for infectious diseases. Until then, the goal of global health security remains an unfinished journey.”
 GMU Biodefense PhD Info Session – October 26th!
GMU Biodefense PhD Info Session – October 26th!
Don’t miss your last chance to catch our biodefense PhD info session before applications are due! On Thursday, October 26th at 7pm at our Fairfax campus, we’ll be hosting this session where you can meet with professors, current students, and find out how much fun getting a PhD can be. Where else can you study everything from synbio to Ebola and even how to stop biological threats? GMU Schar School’s Biodefense program is just the place for all things health security.
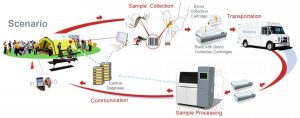
The Worrying State of Epidemic Preparedness & Global Spread of Hemorrhagic Fever Viruses: Predicting Pandemics
University of London professor Sanjeev Krishna studies neglected infectious diseases and like so many, wasn’t surprised at the 2014/2015 Ebola outbreak. He notes that globally, we could’ve been better prepared to handle the outbreak and that vaccine development, among other things, is critical. “At the start of this year an organisation was launched to lead the way, the Coalition for Epidemic Preparedness Innovations (CEPI). Its mission is to bring politicians, academics, drug firms and philanthropists together to help prepare for the next epidemic. It was launched at the World Economic Forum in Davos in January, and is backed with $620m (£466m) from the governments of Norway, Germany, Japan, Canada, Belgium and Australia and the world’s two largest health charities the Wellcome Trust and the Bill and Melinda Gates Foundation. It is working to establish the lab and distribution infrastructure and access to funds needed to rapidly develop vaccines in a crisis.” CEPI Chief Executive Richard Hatchett has continually emphasized the importance of recognizing warning signs and investing in prevention efforts. Hatchett points out that the biggest lesson from Ebola, like so many outbreaks, is that we simply can’t be complacent about diseases with epidemic potential. Vaccine development can take a while and is costly (some say it’s about $1 billion per vaccine) and it’s taken groups like the Bill and Melinda Gates Foundation and Wellcome Trust to really support some of these efforts when government investments have been lacking. These gaps in preparedness and funding are worrisome in the event of a pandemic flu. “Sir John Bell, scientist at Oxford University and author of the UK’s life sciences industrial strategy, agrees on the threat posed by flu, noting that the last flu pandemic in 1918 killed 50m to 100m people, around 3-5pc of the world’s population at the time. ‘The experience of the epidemic in 1919 should give ample cause for concern about the impact of such an event globally,’ he says.” The truth is that we’re still working to prepare and respond to these biological events, but the real question is – will we learn from our mistakes? You can also read Dr. Alaa Murabit’s comments on the challenges of securitizing health and how this UN High-Level Commissioner is tackling global health issues. “Epidemics usually occur when health systems are unprepared.” These words ring especially true this week, during International Infection Prevention week (read below). Hemorrhagic viruses and hantavirus have shown an uncanny ability for epidemic expansion, whether it be through people or rodents across significant geographical areas. “The ultimate goal is to develop a resilient global health infrastructure. Besides acquiring treatments, vaccines, and other preventive medicine, bio-surveillance is critical to preventing disease emergence and to counteracting its spread. So far, only the western hemisphere has a large and established monitoring system; however, diseases continue to emerge sporadically, in particular in Southeast Asia and South America, illuminating the imperfections of our surveillance. Epidemics destabilize fragile governments, ravage the most vulnerable populations, and threaten the global community.” The truth is that we so frequently follow the pattern of poorly prepared health systems responding to epidemics and governments re-alligning preparedness efforts only after the event. The current world is in a state of flux to fix these health issues despite constant external stressors like conflict, growing populations, migration, climate change. Despite these challenges, it is vital we strengthen our health systems to more effectively and efficiently identify biological threats, prevent them, and respond to them.
 Measuring Radiation Doses in Mass-Casualty Emergencies We’re getting a double-dose of GMU biodefense in this fascinating article on radiation measurement. GMU biodefense professor and graduate program director Dr. Gregory Koblentz and doctoral candidate Mary Sproull (who is also a radiation guru at the Radiation Oncology Branch of the National Cancer Institute at the National Institutes of Health) are teaming up to address diagnostic challenges and technologies in the event of a nuclear attack. This article is especially relevant with tensions rising between the United States and North Korea in the wake of nuclear tests. In the event of something this horrific, one of the challenges is to appropriately and accurately diagnosis and treat radiation-related injuries. “Fortunately, new types of diagnostics to address this critical need are being developed in the field of radiation biodosimetry. Radiation biodosimetry is the estimation, through observation of biological variables, of received dose from previous radiation exposure; the new diagnostics use changes in various biological markers to estimate the severity of radiation doses.” Koblentz and Sproull highlight several gaps within U.S. preparedness related to biodosimetry, especially in terms of surge capacity and how such diagnostic capabilities may be challenged in a large-scale event. They also point to research into new assays, like those using newly identified radiation biomarkers. Lastly, Koblentz and Sproull focus on recommendations to better integrate biodosimetry, whether it be integrating medical management of radiation injuries into healthcare provider education or equipping federal response teams with deployable point-of-care biodosimetry diagnostic capability.
Measuring Radiation Doses in Mass-Casualty Emergencies We’re getting a double-dose of GMU biodefense in this fascinating article on radiation measurement. GMU biodefense professor and graduate program director Dr. Gregory Koblentz and doctoral candidate Mary Sproull (who is also a radiation guru at the Radiation Oncology Branch of the National Cancer Institute at the National Institutes of Health) are teaming up to address diagnostic challenges and technologies in the event of a nuclear attack. This article is especially relevant with tensions rising between the United States and North Korea in the wake of nuclear tests. In the event of something this horrific, one of the challenges is to appropriately and accurately diagnosis and treat radiation-related injuries. “Fortunately, new types of diagnostics to address this critical need are being developed in the field of radiation biodosimetry. Radiation biodosimetry is the estimation, through observation of biological variables, of received dose from previous radiation exposure; the new diagnostics use changes in various biological markers to estimate the severity of radiation doses.” Koblentz and Sproull highlight several gaps within U.S. preparedness related to biodosimetry, especially in terms of surge capacity and how such diagnostic capabilities may be challenged in a large-scale event. They also point to research into new assays, like those using newly identified radiation biomarkers. Lastly, Koblentz and Sproull focus on recommendations to better integrate biodosimetry, whether it be integrating medical management of radiation injuries into healthcare provider education or equipping federal response teams with deployable point-of-care biodosimetry diagnostic capability.
Meeting of the Blue Ribbon Study Panel on Biodefense – National Biodefense Strategy: Implementation and Implications
Don’t miss this event at the Hudson Institute on Thursday, November 2nd from 10:30am to 2pm. “This meeting of the Study Panel will address implementation of the National Biodefense Strategy and its implications for the Office of Management and Budget, congressional authorization and appropriation, leadership, coordination, collaboration, and innovation. Thought leaders will draw upon current and previous experiences with implementing national strategies and high-level policy directives. These speakers will also share their thoughts on: (1) the biological threat, the priority they place on biodefense, and efforts to address their concerns; (2) what the Administration should consider as it goes about populating the Implementation Plan for the National Biodefense Strategy; and (3) how Congress should use the Strategy and its Implementation Plan to inform its biodefense oversight and legislative activities.” Make sure to RSVP here by October 30th if you’re attending in person – the event will also be webcast.
Doreen and Jim McElvany Nonproliferation Challenge
Don’t miss out on this wonderful opportunity through the James Martin Center for Nonproliferation Studies (CNS) to encourage innovative thinking and help address nonproliferation. “The James Martin Center for Nonproliferation Studies (CNS) and its journal, the Nonproliferation Review, aim to spur new thinking about nonproliferation and disarmament.To advance this goal, the Doreen and Jim McElvany Nonproliferation Challenge will recognize the most outstanding new ideas and policy proposals published in Volume 25 (2018) of the Nonproliferation Review. The Challenge will award a grand prize of $5,000, a $3,000 runner’s-up prize, and a $1,000 honorable mention prize.”
The Evolution of the Islamic State’s Chemical Weapons Efforts The Islamic State has grown increasingly comfortable with using chemical weapons and Columb Strack is taking us through the evolution of their practices. While their use of chemical weapons seems to have been abandoned since the loss of Mosul in June 2017, intelligence sources have suggested that a new chemical weapons cell has been established within the Euphrates River Valley. “The Islamic State’s use of chemical agents in Iraq and Syria is characterized by three phases. During the initial phase, which encompasses the first year of the caliphate’s existence (between June 2014 and June 2015), chemical attacks drew on tried and tested techniques, adapted to include widely available industrial chemicals—mainly chlorine and phosphine—from stockpiles captured as part of the group’s territorial expansion. These attacks were carried out using crude delivery mechanisms, in most cases adding canisters of chemicals to roadside or vehicle-borne improvised explosive devices (IEDs). The second phase, from July 2015 to January 2017, represents the enhanced capability the group had achieved by combining the production of sulfur mustard agent with the means to deliver it using projectiles, such as mortar bombs and improvised rockets. During this period, chemical attacks were carried out simultaneously across the caliphate, from Syria’s Aleppo province in the west to Iraq’s Kirkuk province in the east, indicating the existence of multiple operational units with the required expertise. Attacks peaked in April 2016, with eight separate recorded chemical attacks in one month. The third phase began with the last recorded chemical attack in Syria on January 8, 2017, and ended with the Islamic State’s apparent abandonment of its CW production following the loss of Mosul in July 2017.” Strack traces the history of intent and methodology development from two decades of experimentation by other militant groups. Strack also discusses experiments and sources for the weapons, including the seizure of military sites where chemical weapons could have been stored. Lastly, he discusses the slow degradation of capability that occurred following airstrikes against facilities and individuals, but that ultimately, the Islamic State has “the capability not only to transfer the know-how to produce toxic chemicals via secure online communications to operatives already living in target countries, but also to ship materials, including explosives, undetected.”
 Blue Ribbon Study Panel on Biodefense- Animal Agriculture Vulnerabilities
Blue Ribbon Study Panel on Biodefense- Animal Agriculture Vulnerabilities
Diseases that impact animals and have the potential to cross over to humans, let alone impact the agriculture industry, can be devastating. The Blue Ribbon Study Panel on Biodefense has just released their report evaluating the threats to animal agriculture and how this can not only impact human health, but also the U.S. economy. “In December 2014, a highly pathogenic strain of avian influenza entered the United States via migrating wild birds. The ensuing outbreak resulted in the largest animal health disaster ever experienced by the United States. Federal and state governments spent $879 million on outbreak response. The outbreak impacted 21 states, lasted until the middle of 2015, and led to the depopulation of more than 50 million birds on 232 farms. Subsequent trade bans impacted as many as 233,770 farms. The total cost to the U.S. economy was estimated at $3.3 billion. In 2015, the agriculture, food, and related industries contributed $992 billion (5.5%) to U.S. gross domestic product (GDP), making it one of the largest sectors of the U.S. economy. Given its critical importance to food safety and availability in the United States and around the world, protecting this sector is a matter of national security.” The report covers the threat to food and agriculture, zoonoses, how federal response is organized, collaborative efforts like biosurveillance, and the innovative work within next-generation medical countermeasures.
Why You Should Be Celebrating International Infection Prevention Week Are you celebrating infection control this week? GMU Biodefense PhD student Saskia Popescu is pointing out how vast the role of infection prevention is across healthcare and why we should all be celebrating it. “October 15-21, 2017 marks International Infection Prevention Week and while this may seem like a week where we rally around hand hygiene, it’s much bigger than that. Infection prevention goes beyond the nuances of hand hygiene and expands to almost every corner of medical care and healthcare. Whether it be a dental clinic, operating room, or even an outpatient treatment center, infection prevention plays a vital role in keeping patients and healthcare workers safe. Not convinced? On any given day, the Centers for Disease Control and Prevention estimates that roughly 25 people in the United States will acquire a healthcare-associated infection (HAI). In a given year, it’s estimated that 722,000 HAIs occur, of which 25,000 of those patients die due to the infection. Realistically, it’s believed that the annual number of HAIs within the United States is closer to 2 million, which is astounding.”
Monkeypox in Nigeria
Nigeria is currently experiencing an outbreak of monkeypox after confirming three cases. “Since Sep 22, there have been 60 reports of suspected monkeypox cases from across Nigeria. The laboratory analysis showed that 12 suspected cases from the Bayelsa state were not positive for monkeypox. The NCDC said that all patients with suspected and confirmed monkeypox are currently receiving supportive medical care and improving. The NCDC offered no further details on the confirmed cases, besides noting that they were from Bayelsa state. The agency said the likely source of infection is through primary zoonotic transmission, and cautioned Nigerians to avoid contact with squirrels, rats, and any animals that appear sick.” Samples are currently being analyzed at the WHO regional office in Dakar, Senegal.
Stories You May Have Missed:
- Did Disease Impact the Fall of Rome?– We know that disease can have devastating consequences on societies and even ancient Rome experienced several outbreaks of smallpox and plague, but just how impacting were these biological events? “Rome was far from the only advanced society shaken to its core by the explosive force of infectious diseases. The medieval Black Death sent some leading-edge polities (like the communities of Italy) backward, while opening the space for the ascent of others, such as England. The lethal role of pathogen exchange in the European conquest of the New World is relatively famous, if still imperfectly understood.”
- Supportive Care Recommendations for Ebola Patients– Treatment for patients afflicted with Ebola can be tricky and there’s often little time to get the right mixture. “The study, by a team of international experts, was published yesterday in The Lancet. The authors write that at the beginning of the outbreak in 2013, case-fatality rates were 70%, but that number was lowered significantly (to 40%) as supportive care practices improved over the course of the outbreak. Using Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology, the authors present evidence-based recommendations for patient care during the next Ebola outbreak. Oral hydration and intravenous hydration had the strongest recommendation. When administered properly, the measure carries no risk of transmission to healthcare workers, the experts say. and making sure patients, especially the very young, are adequately hydrated is a necessary supportive measure.”
Thank you for reading the Pandora Report. If you would like to share any biodefense news, events, or stories, please contact our Editor Saskia Popescu (biodefense@gmu.edu) or via Twitter: @PandoraReport


 Ebola Burial Teams
Ebola Burial Teams 

 Chemical Weapons & ISIS
Chemical Weapons & ISIS Pandemics, Bioterrorism, & Global Health Security Workshop Instructor Spotlight
Pandemics, Bioterrorism, & Global Health Security Workshop Instructor Spotlight
 GAO Report: U.S. Needs To Do More To Prevent Possible Bird Flu Pandemic
GAO Report: U.S. Needs To Do More To Prevent Possible Bird Flu Pandemic




{kind=link}
{kind=link}