
Yowza! That’s another semester in the books for the GMU Biodefense students. Please excuse the sparse activity on the blog, but with the semester over, things should be getting back to normal.
This weekend we have a updates on Ebola and the bird flu outbreak in the U.S., plus other stories you may have missed.
Have a great week, (enjoy the Mad Men finale!) and see you back here next weekend!
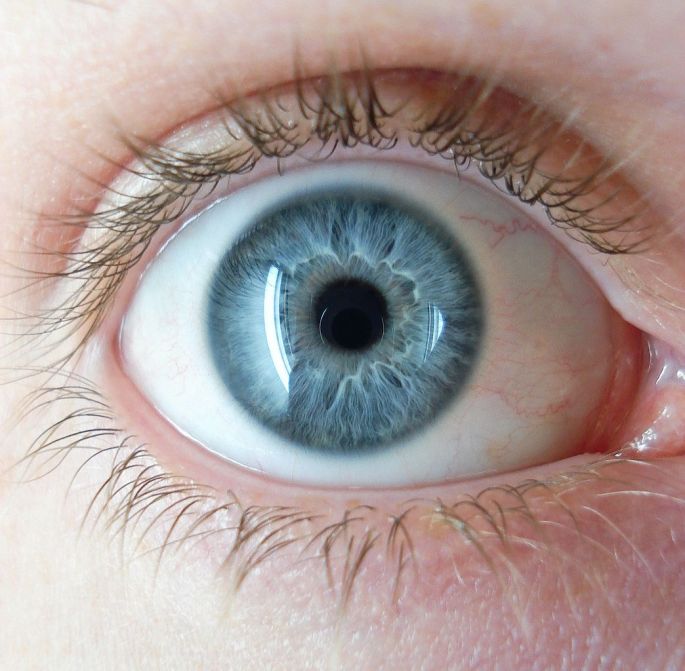
Ebola is (still) living in an American doctor’s eye
As an update, Liberia has (finally) been declared Ebola free, the number of cases in Guinea continue to rise due to transmissions at funerals, and those in Sierra Leone are dying less from Ebola than from other diseases due to the collapse of the healthcare system. It’s been over a year and we are still learning things about Ebola and its persistence on hospital surfaces, sexual fluids, and now, according to a study in the New England Journal of Medicine, the eye. WHO volunteer Ian Crozier was diagnosed in Sierra Leone and transported to Emory University where he was treated. Months later he returned to the hospital with symptoms like blurred vision and acute pain in his left eye. The cause? Ebola.
The Washington Post—“Ebola may have found refuge in patients’ eyes because, researchers said, the eye is walled off from the immune system. As the New York Times put it: “The barriers are not fully understood, but they include tightly packed cells in minute blood vessels that keep out certain cells and molecules, along with unique biological properties that inhibit the immune system.” This phenomenon is called “immune privilege” — and it means the eye can harbor viruses.”
America’s $45 Billion Poultry Industry Has a (Really) Bad Case of Bird Flu
The title says it all, frankly. Since early December 2014 three strains of highly pathogenic avian influenza have been circulating in North America. A state of emergency has been declared in Iowa (one of the hardest hit states) and over 21 million birds have been killed to contain and prevent the spread of the virus. Beyond the culling of birds, the outbreak is having an affect on business—China, South Korea, and Mexico have banned imports of U.S. poultry (to protect their own industries.)
The Motley Fool—“Falling exports could hurt farmers, but it could also help to offset domestic price increases from less supply. Although, with tens of millions of bird deaths and no end in sight to the pandemic, domestic food prices could be the largest casualty in the end.”
Stories You May Have Missed
- Biodefense topics in popular culture (especially TV and movies) are one of my favorite things! That’s why I was delighted to see the medical explanation of Game of Thrones’ greyscale.
- Bird influenza and canine influenza cause problems for our furry and feathered friends, but how can they affect humans? The Washington Post investigates.
- Are you one of the many Americans who takes a daily probiotic? You’ve got Ilya Metchnikoff to thank—the man who drank a glass of cholera all in the name of science!
- Bavarian Nordic pharmaceutical company has announced two successful late-stage tests for a smallpox vaccine called Imvamune.
- I don’t want to shock you, but the OPCW has announced the discovery of chemicals used to make sarin and VX nerve agents at an undisclosed Syrian site. “This is a pretty strong indication [Syria] have been lying about what they did with sarin.”
- According to the U.S. Justice Department a former Department of Energy and Nuclear Regulatory Commission employee has been charged with attempting to extract information on nuclear weapons.
- The WHO received notification that a new case of MERS CoV has been diagnosed in the Islamic Republic of Iran. The 61-year-old patient was treated and discharged.
- The USDA Economic Research Service estimates that the yearly economic burden of foodborne pathogens is $15.5 billion! A run down of the report is available on barfblog (clever name, right?)
Image Credit: 8thstar



{kind=link}
{kind=link}