By Sally Huang, Biodefense PhD Student
Introduction
The COVID-19 pandemic, which was first detected in the Chinese city of Wuhan in December 2019, has turned the world upside down. While the origins of the pandemic, either a natural spillover event from animals to humans or the result of an escaped virus from the Wuhan Institute of Virology, remain contested, there is no denying that the virus has served as a focusing event for political leaders. As a rare, sudden event that has inflicted large-scale harm upon the public, the pandemic has also functioned as a powerful catalyst for policymaking [i]. While China had been drafting new biosafety legislation since 2019, the pandemic accelerated its finalization after President Xi Jinping announced his intent to enhance biosafety measures in February 2020. The law’s approval also comes as China recently experienced one of its worst COVID flare-ups in 2021, challenging the country’s success in overcoming the virus.
On October 17, 2020, China’s Standing Committee of the 13th National People’s Congress approved the Biosafety Law of the People’s Republic of China [ii]. This law is the first of its kind, unifying numerous preexisting biosafety policies under a single framework [iii]. Yet, one may be wary of the law’s credibility in effectively addressing biosafety gaps in China’s infectious disease framework given the political drama surrounding China’s response to the pandemic. China is under heightened scrutiny as the international community questions the origin of the pandemic, China’s initial handling of the COVID-19 outbreaks in Wuhan, and whether Chinese institutions and facilities are prepared to counter future infectious disease threats. Thus, even though China proactively initiated the Biosafety Law to address biosafety concerns, its rapid completion could be seen as a reflexive action to ameliorate the international community’s skepticism. The Biosafety Law’s broad and sometimes vague approach to addressing pathogen management, biohazardous agent accountability, capacity-building, and preparedness also highlight that there is much work to be done beyond approval of the law.
China’s Biosafety Law is unlike a highly detailed US law. Rather, it is analogous to a US government-issued strategy, a high-level document setting forth broad principles for subsequent legislative actions and policies. Thus, Chinese ministries will have to subsequently provide additional details to build upon the Biosafety Law. While strategy documents retain a certain amount of ambiguity to set the stage for more prescriptive, future policies, China’s Biosafety Law exhibits a noticeable lack of clarity. An analysis of the Biosafety Law’s key elements will therefore help inform outside parties about how China plans to navigate the infectious disease and biotechnology landscape moving forward.
Prior to diving into China’s Biosafety Law, it is worth taking a few moments to describe the linguistic differences between how Western and Chinese scientific communities use the terms, biosafety and biosecurity. When using these terms, the Western scientific community references two separate, but interrelated disciplines. The Chinese scientific community commonly uses the term shengwu anquan (biosafety) while also presently developing familiarity with shengwu anbao (biosecurity). Due to the widely varying opinions on what biosecurity means depending on where one works, Chinese scientists characterize shengwu anbao (biosecurity)as a subcategory of shengwu anquan (biosafety) as opposed to an independent field of study. An unintended consequence of this is the Chinese scientific community’s tendency to use these terms interchangeably [iv]. This may be a result of China’s intent to grow their biosecurity sector under the aegis of their biosafety policies, which were made more comprehensive following the country’s 2003 SARS outbreak [v]. On the other hand, this may cause confusion to the unbeknownst reader. In an effort to best maintain the Biosafety Law’s context in this article, the evaluation below adopts China’s interpretation of biosafety and biosecurity. Therefore, readers should keep in mind that as biosecurity (as described below) encompasses the security of biotechnologies, it is applied in the context of biosafety.
China’s Biosafety Law: Why Now?
COVID-19 highlighted the absence of a central agency and legal framework in China to provide direction for policies related to the management of threats posed by infectious diseases and biotechnology. Even with nearly a hundred existing biosafety laws and regulations, China has struggled with communicating, coordinating, and enforcing biosafety regulations. This demonstrates that a variety of policies can foster inconsistencies and poor policy oversight [vi]. As a result, China’s regulations are problematically left open to interpretation by all levels of government [vii]. Left unattended, these issues could balloon into long-term complications that could disrupt or contradict efforts to combat infectious diseases. Thus, China’s new Biosafety Law is meant to unify preexisting biosafety policies under one single framework to promote national biosafety standards and regulations, and demonstrate to the world their commitment to improving biosafety practices and infectious disease preparedness.
What Does the Biosafety Law Aim to Do?
Comprised of 88 articles, China’s Biosafety Law aims to bolster prevention and response to the threat of biological agents, nurture responsible laboratory conduct, and promote stable development of biotechnology to ensure the well-being of the ecosystem and population. As a basic, all-encompassing law, it takes a broad approach to formulating supervisory parameters for various issues of concern beyond biosafety and biosecurity. It bestows the Chinese State Council—the executive body of state power in charge of carrying out policy—with the authority to enforce, oversee, and lead investigations for all activities addressed under the law [viii]. With the Biosafety Law serving as the chief blueprint, it will work towards integrating various areas to fortify national and economic security, and social stability as well as set a precedent for future policies. The main components of China’s Biosafety Law include biosafety, biosecurity, public health preparedness, ethics, and biodefense.
Biosafety Prevention and Standards
China defines biosafety as the effective prevention and response to threats of biological agents and related factors to peoples’ lives and the ecosystem, and the stable development of biotechnologies [ix]. Although the law lists various areas in which biosafety would apply, it does not clearly define laboratory safety procedures or implementation of containment principles in the event that accidental outbreaks were to take place. This is interesting as the Western definition of biosafety more clearly lists criterion and values for protecting lab personnel and the public from the threat of biological agents [x]. However, it is worth noting that biosafety is explicitly written as “an important part of national security” within the Law as numerous articles describe the boundaries of biosafety activities and appropriate behavior in China [xi]. Article 6, for example, emphasizes the need to strengthen international cooperation and fulfill biosafety obligations under international treaties. This is especially pertinent to China’s compliance to the Cartagena Protocol on Biosafety in order to improve governance over the movement of pathogens and modified organisms [xii].
Article 8 empowers individuals to report activities endangering biosafety with the goal of preventing government authorities from ignoring early warning signs and valuable information provided by experts. This is a significant provision that could provide protection for whistleblowers. During the earliest stage of the COVID-19 outbreak in Wuhan, for example, Dr. Li Wenliang, a doctor treating patients with the novel coronavirus was detained and reprimanded by Chinese authorities for raising alarms about the hazards of the virus via social media. After his death from contracting COVID-19, he was hailed as the “hero who told the truth” as the Chinese public became outraged over the initial cover-up and number of lives that could have been saved if authorities had heeded the warnings [xiii]. The inclusion of this provision should pose a sanguine outlook for whistleblower protections, but specific assurances are not described. Only time will tell how Chinese government officials will act in the future.
The biosafety-focused articles also promote joint agency collaboration to enhance biosafety capacity-building. Article 42 stipulates that China should formulate a unified biosafety standard for pathogenic microorganisms in laboratories. Article 45 establishes hierarchical management for biosafety laboratories (BSLs) to ensure that research on pathogens is carried out responsibly in appropriate BSLs as categorized by risk level. Expanding upon responsible operation of pathogens, Article 68 calls for construction of a national biosafety infrastructure to accommodate high-grade pathogens and bolster national preparedness and response. As of now, China has only two BSL-4 labs [xiv]. The Biosafety Law does not dictate which types of biocontainment labs will be built. However, China is reportedly planning on building thirty additional BSL-3 labs and at least one BSL-4 lab over the next five years [xv].
Most reflective of the COVID-19 environment is Article 70 which details the State Council’s role in ensuring “the production, supply and deployment of medical rescue equipment, treatment drugs, medical devices and other materials needed for emergency response to biosafety incidents” [xvi]. Like any other country combatting COVID-19, healthcare workers and first responders in China are on the frontlines and require proper protective gear and medical countermeasures to help those in need.
Public Health and One Health
With the pandemic sparking additional concerns about novel infectious disease outbreaks, multiple provisions of the law address public health concerns. Article 18 dictates China will establish a biosafety inventory system to catalogue important biological data, including animal and plant, and other invasive species. Article 15’s biosafety risk investigation and evaluation system, combined with Article 16’s unified national biosafety information sharing system, will then help identify animal and plant epidemic risks that endanger China’s biosafety. China is also poised to streamline communication between government departments to efficiently classify and manage potential outbreaks. Article 47 aims for more controlled management of experimental animal research in laboratories to better protect the public. These articles reflect China’s efforts to amend loopholes in its public health and biosafety systems after SARS escaped Beijing labs twice in 2004. Continued speculation of the origin of COVID-19 also places pressure upon China to straighten their public health systems.
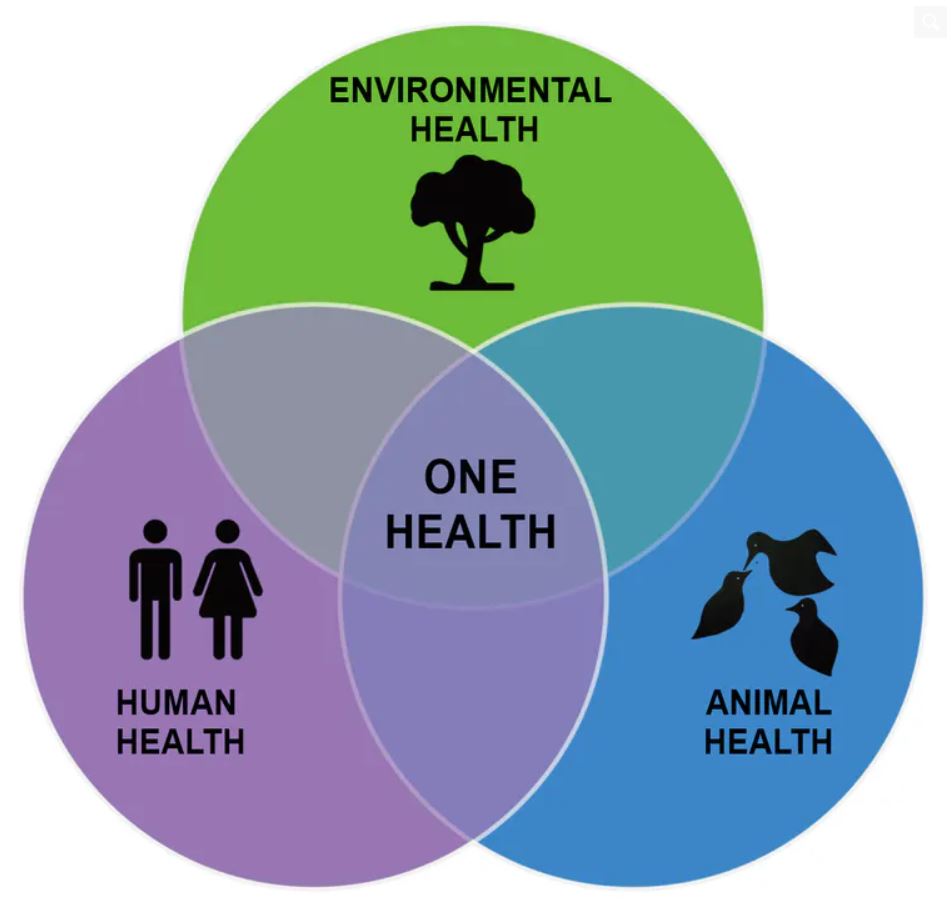
Articles 22, 23, and 27 through 30 have a One Health focus—an interdisciplinary approach that recognizes the intersection between human, plant, and animal health [xvii]—and dedicate attention to the development of monitoring systems to trace and manage epidemics among plants and animals. Article 31 stresses the importance of strengthening capacity building measures for prevention and control of animal and plant agents at borders and ports. Article 32 expresses China’s aim to protect wildlife and prevent the spread of infectious diseases of animal origin. This will be vital for countering infectious diseases that are approximately 60-75% zoonotic [xviii]. To further champion animal and plant epidemic protections, Article 60 sets out to formulate lists of invasive alien species as guides for creating relevant management measures. By taking a One Health approach to recognizing and reducing infectious disease threats, these articles demonstrate China’s hope in preserving biodiversity, ecosystems, and the natural environment.
Security of Biotechnology Research and Applications
The Biosafety Law does not include a definition for biosecurity. Instead, biosecurity is considered a part of biotechnology dual-use research of concern (DURC). China’s singular attention to biosafety after the 2003 SARS outbreak meant that the Chinese scientific and legislative community did not become familiar with biosecurity until later on [xix]. According to Michael Barr, there are widely varying opinions on biosecurity in China and there is a “divergence of awareness” [xx] depending on where one works, but biosecurity is generally considered a subcategory of biosafety. This differs from the Western scientific community’s interpretation of biosecurity, in which biosafety and biosecurity are separate, but complementary, disciplines.
Recognizing the role of DURC in biotechnologies and how it influences pathogen management, Article 34 strengthens the safety management of biotechnology research while prohibiting research activities that endanger public health and damage ecosystems or biodiversity. Article 36 seeks to formulate biotechnology R&D standards and classifies biotechnology R&D activities as high-risk, medium-risk, and low-risk “according to the degree of risk of harm to public health, industrial agriculture, ecological environment, etc” [xxi]. Article 39 emphasizes the importance of regulating the purchase and introduction of biotechnologies and related biological factors in accordance with a control list and prohibits individuals from purchasing or possessing items on this list. The law does not provide any details on the contents of this control list.
Ethics
The Biosafety Law also covers ethical issues such as how China should improve supervision of Human Genetic Resources (HGRs). The ethical handling of HGRs has become an important issue in China after Dr. He Jiankui used CRISPR technology to produce gene-edited babies in an attempt to reduce their susceptibility to HIV [xxii]. This controversial experiment raised a number of red flags for the international scientific community—not only was it a flagrant flouting of medical and research ethics, but it also evinced China’s ineffective regulations and scientists’ lack of compliance. Therefore, Article 53 calls for strengthened supervision of the collection, preservation, and utilization of HGRs and related biological resources. Article 54, which empowers the State Council to carry out necessary investigations, provides a means of verifying compliance with these new provisions. Details on how the State Council would conduct these investigations, however, are not provided. Nonetheless, the universally negative response to Dr. He’s experiment provided a strong incentive for China to redefine its HGR regulations and reshape its bioethics standards.
Promoting Biodefense
Through Article 61 of the Biosafety Law, China hopes to “take all necessary measures to prevent biological terrorism and the threat of biological weapons”[xxiii]—echoing the Biological Weapons Convention’s (BWC) objective of prohibiting the development, manufacture, acquisition, stockpiling, possession, and utilization of biological weapons [xxiv]. China has already passed legislation for domestic implementation of the BWC and reported its biosecurity policies and enforcement measures to the United Nations Security Council’s 1540 Committee. In 2019, however, the US State Department reported that China was engaged in “biological activities with potential dual-use applications, which raises concerns regarding its compliance with the BWC” [xxv].
Article 62 tasks the State Council with creating China’s own version of the US’s Select Agent and Toxins List which is used to regulate access to dangerous pathogens that could be used by terrorists. Though criteria for this list are not described, a biological agent control list would provide China with a more formal method for managing, monitoring, and investigating suspicious purchases or activities with biological agents at risk of being misused to cause harm. Meanwhile, Article 65 calls for investigations of remnants of biological weapons found within China and the construction of facilities for their storage and disposal. The discovery and disposal of abandoned biological weapons holds historical significance for China as the country was subjected to multiple biological attacks by Japan during the Sino-Japanese War, and Chinese prisoners of war and captured civilians were victims of Japanese BW experiments conducted by Unit 731 in Manchuria during this time [xxvi]. At the end of the war, Japanese abandoned the site and destroyed records. However, recent discoveries of new records and an incubator used for the production of Yersinia pestis (the causative agent for plague) at sites in China indicates that the destruction of Unit 731’s equipment and materials was not completely thorough [xxvii]. Thus, other experimental equipment and biological munitions have the potential to be unearthed. These efforts to clean up the legacy of Japan’s biological weapons program in China complements China’s long-standing effort to safely destroy abandoned Japanese chemical weapons [xxviii].
Penalties for Violating the Biosafety Law
The Biosafety Law concludes with a final chapter on penalties for individuals who violate the law through the abuse of power, neglect of duties, engagement in malpractice for personal gain, fabrication of false information, and/or criminal acts. Penalties for such violations are financial fines that range between thousands to millions of yuan depending on the scope of the violation committed. The law does not delineate any prison time or any other form of penalties distinct from financial fines. With these current penalties, China hopes to influence scientific institutions and personnel to comply with the Biosafety Law. Yet, these articles do not describe pertinent criminal laws that would apply nor does it address whether novel criminal laws will be created to enforce the Biosafety Law—leaving the parameters for legal responsibility and investigations ambiguous.
Conclusion
Even as the Biosafety Law reflects China’s strategic positioning to incorporate biosafety, biosecurity, and biotechnology into its national security system, this ambitious set of laws needs to be accompanied by verification and accountability measures to ensure its proper implementation. What’s more, it will be interesting to see how China’s new expansive benchmarks will hold up, especially as the wording of key articles may be too broad and vague to be interpreted clearly. Nevertheless, countering infectious disease threats will be a balancing act requiring steadfast commitment and investment. COVID-19 has served as a long-awaited wake-up call for China to re-center their policy efforts and develop purposeful strategies to reduce the threats posed by natural and man-made biological threats. As the world continues to face infectious disease threats, the Biosafety Law serves as a preliminary touchstone for Chinese scientists and institutions to elaborate upon. This new law is the beginning of a long process of heightening biosafety from a local concern to a national one and developing the policies, processes, and institutions necessary to implement the law. Only then can the Biosafety Law begin to be the comprehensive and effect
[i] Thomas A. Birkland, Lessons of Disaster: Policy Change after Catastrophic Events, American Governance and Public Policy Series (Georgetown University Press, 2006), https://www.jstor.org/stable/j.ctt2tt2sn.
[ii] Biosafety Law of the People’s Republic of China, October 17, 2020, http://www.npc.gov.cn/npc/c30834/202010/bb3bee5122854893a69acf4005a66059.shtml
[iii] Shihui Qiu and Ming Hu, “Legislative Moves on Biosecurity in China,” Biotechnology Law Report 40, no. 1 (January 21, 2021): 27–34, https://doi.org/10.1089/blr.2020.29217.mh.
[iv] Michael Barr, “Cures That Kill,” China Security 4, no. 4 (2008): 33–42.
[v] Gigi Kwik Gronvall, Matthew Shearer, and Hannah Collins, National Biosafety Systems: Case studies to analyze current biosafety approaches and regulations for Brazil, China, India, Israel, Pakistan, Kenya, Russia, Singapore, the United Kingdom, and the United States (Baltimore, MD: UPMC Center for Health Security, July 2016), 8.
[vi] Jia Li and Yunfeng Jing, “Biosecurity Law — A Landmark Law to Be Released Soon,” China Law Insight, October 20, 2020, https://www.chinalawinsight.com/2020/10/articles/biolaw/biosecurity-law-a-landmark-law-to-be-released-soon/.
[vii] Barr, “Cures That Kill.”
[viii] “The State Council,” accessed February 6, 2021, http://en.people.cn/data/organs/statecouncil.shtml.
[ix] “Biosafety Law of the People’s Republic of China” (China National People’s Congress, October 17, 2020).
[x] Judi Sture, Simon Whitby, and Dana Perkins, “Biosafety, Biosecurity and Internationally Mandated Regulatory Regimes: Compliance Mechanisms for Education and Global Health Security,” Medicine, Conflict, and Survival 29, no. 4 (2013): 289–321, https://doi.org/10.1080/13623699.2013.841355.
[xi] “Biosafety Law of the People’s Republic of China.”
[xii] Biosafety Unit, “Parties to the Cartagena Protocol and Its Supplementary Protocol on Liability and Redress,” The Biosafety Clearing-House (BCH) (Secretariat of the Convention on Biological Diversity, March 5, 2018), https://bch.cbd.int/protocol/parties/.
[xiii] Verna Yu, “‘Hero Who Told the Truth’: Chinese Rage over Coronavirus Death of Whistleblower Doctor,” The Guardian, February 7, 2020, http://www.theguardian.com/global-development/2020/feb/07/coronavirus-chinese-rage-death-whistleblower-doctor-li-wenliang.
[xiv] World Health Organization, WHO Consultative Meeting on High/Maximum Containment (Biosafety Level 4) Laboratories Networking: Meeting Report (World Health Organization, 2018), http://www.who.int/ihr/publications/WHO-WHE-CPI-2018.40/en/.
[xv] Frank Chen, “China Goes on Biosafety Lab Building Spree,” Asia Times, July 7, 2020, https://asiatimes.com/2020/07/china-goes-on-biosafety-lab-building-spree/.
[xvi] “Biosafety Law of the People’s Republic of China.”
[xvii] “One Health Basics,” Centers for Disease Control and Prevention, November 5, 2018, https://www.cdc.gov/onehealth/basics/index.html.
[xviii] Stephanie J. Salyer et al., “Prioritizing Zoonoses for Global Health Capacity Building—Themes from One Health Zoonotic Disease Workshops in 7 Countries, 2014–2016,” Emerging Infectious Diseases 23, no. Suppl 1 (December 2017): S55–64, https://doi.org/10.3201/eid2313.170418.
[xix] Amy E Smithson, Monterey Institute of International Studies, and James Martin Center for Nonproliferation Studies, Beijing on Biohazards: Chinese Experts on Bioweapons Nonproliferation Issues (Monterey, Calif.: James Martin Center for Nonproliferation Studies (CNS). Monterey Institute of International Studies, 2007), 47, http://cns.miis.edu/reports/pdfs/beijing_on_biohazards.pdf.
[xx] Barr, “Cures That Kill.”
[xxi] “Biosafety Law of the People’s Republic of China.”
[xxii] David Cyranoski, “What CRISPR-Baby Prison Sentences Mean for Research,” Nature 577, no. 7789 (January 3, 2020): 154–55, https://doi.org/10.1038/d41586-020-00001-y.
[xxiii] “Biosafety Law of the People’s Republic of China.”
[xxiv] “The Biological Weapons Convention (BWC) At A Glance | Arms Control Association,” Arms Control Association, accessed January 20, 2021, https://www.armscontrol.org/factsheets/bwc.
[xxv] Richard Pilch, “Engaging China on Bioweapons and Beyond,” James Martin Center for Nonproliferation Studies, May 28, 2020, https://nonproliferation.org/engaging-china-on-bioweapons-and-beyond/.
[xxvi] Sheldon H. Harris, Factories of Death: Japanese Biological Warfare, 1932-45 and the American Cover-Up, 2nd edition (New York: Routledge, 2002).
[xxvii] “China Reveals New Evidence of Japan’s Germ War Atrocities,” Xinhua Net, August 18, 2017, http://www.xinhuanet.com//english/2017-08/18/c_136536353.htm.
[xxviii] Wanglai Gao, “Unearthing Poison: Disposal of Abandoned Chemical Weapons in China,” Bulletin of the Atomic Scientists 73, no. 6 (November 2, 2017): 404–10, https://doi.org/10.1080/00963402.2017.1388678.