Summer Workshop Cancellation
We are so grateful for all the interest in the workshop over the years, but regretfully have decided to cancel the 2020 workshop due to the ongoing COVID-19 pandemic. In the interest of public health, George Mason University has cancelled all on-campus events through mid-August. We hope you and your family stay healthy and safe. If you are working on the response to COVID-19, we would like to thank you for your hard work and dedication to global health security. We are confident that the 2021 workshop will offer critical insights into the causes and consequences of this pandemic and a renewed passion for biodefense efforts. We hope to see you at next summer’s workshop and thanks to all for their interest.
 ‘Understanding and Surviving a Pandemic’ A Week of Scholarly Webinars
‘Understanding and Surviving a Pandemic’ A Week of Scholarly Webinars
From April 27-May 1, 2020, you can enjoy a daily virtual event with a range of experts on the implications of the COVID-19 pandemic. Each day, a panel of experts from the Schar School of Policy and Government at George Mason University, guest practitioners, and elected officials will examine a different aspect of the coronavirus crisis, from politics to health care to intelligence. Mark J. Rozell, dean of the Schar School, will host the programs. The virtual sessions are open to the public and may be followed by a question and answer period, if time allows. See below for topics, times, and viewing information. Don’t miss the Tuesday event on infection control and surge capacity with Biodefense doctoral alum Saskia Popescu. You can read about the events and register for each webinar here.
Schar School Event- Public Policy in the Pandemic Age: How COVID-19 is Reshaping our Government, Economy, and Society
Join the Schar School Faculty, Alumni, Schar Alumni Chapter, and Dean Mark Rozell for an engaging virtual panel on the future of public policy post COVID-19 – COVID-19: How the Pandemic is Reshaping our Government, Economy, and Society. This virtual event will be held from 2-3:30pm EST on Wednesday, May 20, 2020. The COVID-19 pandemic is presenting unprecedented challenges to the United States and the rest of the world. Not since the “Spanish Flu” of 1918 have we experienced a pandemic of this scale and severity. Aside from the steep and growing human toll of the outbreak, virtually every aspect of our personal and professional lives are being affected. The sheer breadth of issues impacted by COVID-19 is overwhelming: public health, medicine, government, the economy, international trade, education, national security, politics, and technology, to name just a few. The effects of the pandemic are also magnified by existing cleavages within our society ranging from hyperpartisanship to racial disparities to socioeconomic inequalities. You can read more about our distinguished panel members and register for the event here.
Recent Developments in White Supremacist Terrorism
GMU Biodefense doctoral student Stevie Kiesel discusses a security threat that we might be overlooking right now. Steve notes that while the national focus has correctly shifted to the threat from COVID-19, other national security threats have not gone away. On the contrary, domestic and international terrorist groups view the pandemic as a chance to sow chaos and strike at their vulnerable enemies. The Voice of Hind, a magazine supportive of the Islamic State and published in India, recently called on supporters to “use this opportunity to strike [nonbelievers] with a sword or a knife or even a rope…[and] fill the streets with their blood.” Closer to home, on March 24, Timothy Wilson accelerated his plan to deploy a vehicle-borne improvised explosive device to cause mass casualties. Recognizing an opportunity to use the pandemic as a force multiplier, Wilson was on his way to his target—a crowded Missouri hospital—when he was intercepted by the FBI. Wilson had been the subject of a domestic terrorism investigation for his “violent extremist” ideology that was “motivated by racial, religious, and anti-government animus.” Read more here.
Counting Calories in COVID-19
GMU Biodefense doctoral student Rachel-Paige Casey discusses COVID-19 implications for food shortages, American food culture, and what widespread stay-at-home orders mean for our diets. “To assuage any panic, the outlook for domestic food production – namely in cereals, meat, and dairy – remains sufficient despite reduced production. A recent announcement by Robert Johansson, USDA Chief Economist in Food and Nutrition, confirms that the United States possesses sufficient quantities of food to feed our population and maintain much of its exports. Anxiety averted and assuaged, patience is needed as our food value and supply chains adapt to abrupt changes in demand. Additionally, the agricultural and food processing sectors need time to adjust operations to increase safety measures (for its workers and customers) and to fulfill changes in consumer preferences.” Read more here.
OPCW Confirms Syrian Sarin Chemical Weapon
The Organisation for the Prohibition of Chemical Weapons (OPCW) published its First Report by the Investigation and Identification Team (IIT), which strongly linked the Syrian government to the March 2017 sarin and chlorine attacks on a rebel town. Specifically, in March 2017, three projectiles – two containing sarin and one containing chlorine – were dropped from aircraft of the Syrian Arab Air Force into Ltamenah in northern Syria. According to Dr. Gregory Koblentz, Dirrector of the Biodefense Graduate Program and member of the Scientists Working Group on Chemical and Biological Security, the IIT’s use of multiple methods provided “damning evidence” of that the sarin was developed by the Syrian government. Unfortunately, the IIT does not have the authority to issue sanctions against Syria as punishment. Kenneth D. Ward, US ambassador to the OPCW, assured that the use of chemical weapons will not be tolerated by the United States, which will seek to hold Syria accountable.
 COVID-19 and International Security Podcast
COVID-19 and International Security Podcast
Have you heard the latest Power Problems podcast episode? You can listen to Dr. Greg Koblentz of George Mason University as he joins Emma Ashford and Trevor Thrall to talk about the international security implications of the coronavirus pandemic. This is an engaging and insightful podcast that discusses national security in the age of pandemics and how we govern in a crisis, let alone reconsidering biosecurity and a recalibration of our efforts during biological threats. As Koblentz reiterates, “This pandemic should be a wake-up call to the national security community that its time to rethink its priorities. Instead of obsessing about great power competition, we should be more focused on defeating our microscopic enemies. When great powers compete over global health, the only winners are the viruses.”
The “Best People” for Pandemic Response? Vaccine Expert Leaves BARDA While Labradoodle Breeder Leads HHS COVID-19 Efforts
From critical vacancies to questionable personnel choices, this week has been another shaky one for the White House. And no, we’re not referring to comments about injecting disinfectants into the body to prevent COVID-19… On Wednesday, a startling shakeup occurred- Dr. Rick Bright was removed from his position as director of BARDA. Not one to go quietly, Bright released a statement stating that leadership pressured him to look more into hydroxychloroquine despite concerns. “I believe this transfer was in response to my insistence that the government invest the billions of dollars allocated by Congress to address the Covid-19 pandemic into safe and scientifically vetted solutions, and not in drugs, vaccines and other technologies that lack scientific merit,” he said in his statement. “I am speaking out because to combat this deadly virus, science — not politics or cronyism — has to lead the way.” Unfortunately, this wasn’t the only shake-up in how the U.S. is responding to COVID-19. Despite President Trump stating that he only hires the best people, it turns out that the aide of HHS Secretary Alex Azar, was tapped to take over COVID-19 response for the agency despite his lack of experience in public health and a track record for…dog-breeding. “The aide, Brian Harrison, had joined the department after running a dog-breeding business for six years. Five sources say some officials in the White House derisively called him ‘the dog breeder.’ Azar’s optimistic public pronouncement and choice of an inexperienced manager are emblematic of his agency’s oft-troubled response to the crisis. His HHS is a behemoth department, overseeing almost every federal public health agency in the country, with a $1.3 trillion budget that exceeds the gross national product of most countries.” GMU Biodefense graduate program director Dr. Gregory Koblentz emphasized these key personnel vulnerabilities in this 2017 OpEd and the implications for biodefense.
The World vs. COVID-19: Potential Models for Stymying the Spread of COVID-19
Michael Krug, a soon-to be-graduate of the Biodefense MS program, was recently hired on by HHS’s Office of Global Affairs as a Global Health Officer for the Office of Pandemics & Emerging Threats. As a budding biodefense professional, the Pandora Report reached out to Krug for his thoughts on his upcoming career and how the GMU Biodefense Graduate Program helped him land his new role. “The Biodefense Program at GMU helped hone my policy knowledge on several topics significant to my work now, including global health policy, health security, and international norms. The program’s proximity to Washington, DC enabled me to find meaningful work experience, to go along with the robust policy-oriented curriculum. One of the reasons I joined the Office of Global Affairs (OGA) at HHS was to help support the core efforts and expertise that strengthen global health priorities. The OGA promotes coordination and partnership between all levels of governments, international and non-governmental organizations. Together these efforts highlight the importance of global health and raise awareness to the health risks around the world. In this interconnected world, I felt as though the OGA provided me the greatest opportunity to make a resounding impact on the global health field.” Krug recently published an article for GMU’s Center for Security Policy Studies about strategies and countermeasures for stymy the continued spread of COVDI-19, citing South Korea and Washington state as examples. Please read Krug’s latest article here.
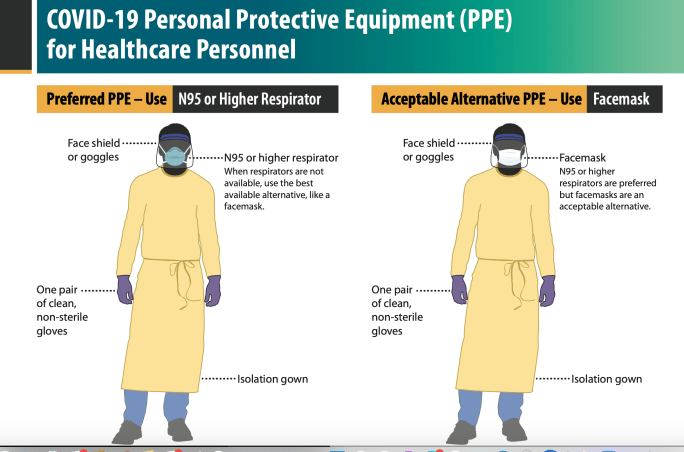
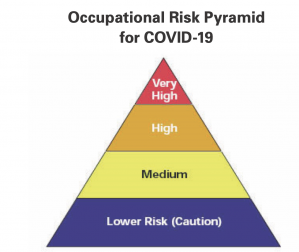 Realigning the conventional routes of transmission: an improved model for occupational exposure assessment and infection prevention
Realigning the conventional routes of transmission: an improved model for occupational exposure assessment and infection prevention
GMU Biodefense doctoral alum Chris Brown is addressing the very real challenges of occupational exposure assessments, which couldn’t come at a better time as we learn about more healthcare-related COVID-19 cases. “Current recommendations for standard and transmission-based precautions in place for patients who are suspected or known to be infected or colonized with infectious agents are best suited to prevent the transfer of micro-organisms to other patients – that is, to prevent the acquisition of a healthcare-associated infection, rather than to protect the healthcare worker from self-contamination resulting in a potential occupationally acquired infection. This article reviews current recommended infection prevention and control practices and offers a framework for better protection and controls from an occupational health point of view. We offer a model with two exposure routes – contact and aerosol – resulting from work activities and environments, shifting the focus away from particular pathogenic micro-organisms’ typical methods for spreading to patients or to other non-workers in hospital and community settings.” Read more here.
ASPR’s Activities
The office of the Assistant Secretary for Preparedness and Response (ASPR) is housed in the Department of Health and Human Services (HHS) and was established by the created under the Pandemic and All Hazards Preparedness Act (PAHPA) in 2006. The ASPR manages the Strategic National Stockpile (SNS) of medical supplies, personal protective equipment (PPE), medicines, and devices for life-saving care in an emergency situation. In the COVID-19 response, the SNS has distributed PPE (N95 respirators, surgical and face masks, face shields, gloves, and disposable gowns) in all 50 states to help subdue the transmission of COVID-19; it has also provided ventilators to areas with critical need. The SNS, in conjunction with its federal partners, is coordinating logistics operations to optimize all available resources to support the COVID-19 response. HHS launched the ASPR Technical Resources, Assistance Center, and Information Exchange (TRACIE) to “meet the information and technical assistance needs of regional ASPR staff, healthcare coalitions, healthcare entities, healthcare providers, emergency managers, public health practitioners, and others working in disaster medicine, healthcare system preparedness, and public health emergency preparedness.” TRACIE covers healthcare coalitions, CBRN, health care system partners and medical surge, the Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers (CMS EP Rule), hurricanes, disaster behavioral health, mass violence, infectious diseases, drug shortages and scarce resources, and emergency medical services (EMS). TRACIE’s COVID-19 page highlights the resources developed and identified to aid ongoing response and recovery operations.
COVID-19 Testing: Possibilities, Challenges, and Ensuring Equity (NAS)
This week, the National Academies of Sciences and the American Public Health Association hosted a webinar about COVID-19 testing and its equity issues. The presenters provides an update on the state of testing for COVID-19, explained the types of data that will be provided by different tests under development, discussed how that data can inform plans to ease social distancing, and described the equity issues that must be considered access testing and how we can ensure equal access for all. The panel experts included moderator David Relman, MD, Professor of Microbiology and Immunology at Stanford University; Jill Taylor, PhD, Director of the Wadsworth Center for the New York State Public Health Department; Ashish Jha, MD, MPH, Director of the Harvard Global Health Institute; and Georges C. Benjamin, MD, Executive Director of the American Public Health Association. Notes and slides for this and related events are available here. The panel covered situational awareness of diagnostics and surveillance, FDA-approved and EUA-approved molecular and serology assays for testing, the accuracy and reliability of existing tests, ongoing studies for new diagnostics, and, of course, the inequities of the current testing strategy. Diagnostics, using any type of test, need to provide data and insight about active SARS-CoV-2 infections, stage of infection, symptom level (or asymptomatic), contagiousness, prognosis, clinical needs, and acquired immunity. Surveillance systems need to provide data and insight about acquired immunity, susceptibility, geographic and temporal factors for infection, and the efficacy of intervention measures. The slow and meager early response efforts of the US were seen in the lack of testing infrastructure, an insufficiency that persists weeks later. The high positive rate (about 20-22%) of US diagnostic testing signals that testing coverage is inadequate as many other nations who have expanded their testing network see positive rates under 10%. There are two camps about the number of tests per day that are needed to achieve reasonable containment of the virus in the US: 500,000/day or 10-30 million/day. The 500,00 tests per day recommendation is probably the only attainable option. Beyond reaching that figure, testing needs to be economically accessible to all subpopulations that are currently struggling to get testing or care. At present, the coronavirus test is covered by the federal government; however, the cost of the appointment and the proceeding care are not, which is a major obstacle for Americans that lack sufficient insurance coverage or a nearby care facility. Dr. Benjamin pointed out that current public health messaging campaigns are focused on television and social media platforms that are not accessible to everyone, but neglects using the radio as a platform for PSAs and information. Additionally, some of the innovations are only applicable certain groups; drive-thru testing sites are a novel option but only for those who own a car. Dr. Benjamin also recommends using locally trusted messengers, such as faith leaders, for public health communication. The aforementioned health inequities are not new occurrences but are of critical concern as we try to combat COVID-19. If we can quickly and adequately enhance our testing strategy to scale up testing and expand accessibility to underrepresented subpopulations, we should finally be able to contain the virus enough to slowly and safely start resuming “normal” life.
 Cascading Economic Impacts of the COVID-19 Outbreak in China
Cascading Economic Impacts of the COVID-19 Outbreak in China
The US-China Economic and Security Review Commission released a Staff Research Report on the economic impacts of COVID-19 in China. China’s late response to the originally-localized outbreak in Wuhan province led the Chinese government to unforce lockdowns across the country, crippling economic activity. With respect to the COVID-19 pandemic, the Commission found that China suffered, and continue to grapple with, obstructed demand in energy and retail items, stalled production and exports, supply chain disruptions. The Chinese supply chain disruptions are impacting global supply chains, and the US is seeing the effects. These interruptions in economic activity are also the result of intentional freezes by Chinese policymakers in an attempt to curtail the spread of the virus while maintaining supply-side efforts to support businesses; this attempt is largely considered a failure. The ultimate result of China’s slow yet extreme response measures is a deceleration of international economic activity. The International Monetary Fund (IMF) now forecasts a 3% global GDP contraction in 2020. The IMF estimate is somewhat optimistic as it relies on the assumptions that pandemic subsides and other support will be enacted in most countries during the second quarter of 2020 and economic activity will mostly resume in the latter half of this year. The full report is available here.
OHSS Webinar – Wildlife trade: the social, cultural, and political stakes
The One Health Social Sciences Initiative is hosting a webinar on April 30, 2020 from 11am-12:30pm EST, with two experts in zoonotic epidemics in an inter-disciplinary dialogue about the social, cultural, and political stakes of eliminating the wildlife trade and, in particular, the role of “wet markets”. Dr. Laura Kahn and Dr. Christos Lynteris will be the speakers of this engaging event. As the potential breeding ground for the current worldwide COVID-19 pandemic, epidemiologists, public health officials, and wildlife conservationists have called for shutting down these markets. However, as a central means of sustenance for many communities around the world, the full impacts of closing the markets and necessary strategies to address them will be addressed. Register for this free event here.

 Summer Workshop on Pandemics, Bioterrorism, and Global Health Security
Summer Workshop on Pandemics, Bioterrorism, and Global Health Security