National Security in the Age of Pandemics
This week, Dr. Gregory Koblentz, Director of the Biodefense Program, and Dr. Michael Hunzeker, Associate Director of the Center for Security Policy Studies, published a commentary asserting that pandemic preparedness cannot be improved if it becomes another item on the military’s infinite laundry list of missions and threats. The COVID-19 outbreak on the USS Theodore Roosevelt forced the ship’s commander to temporarily scale back operations it so that its crew could isolate themselves and later resume their duties after subduing the infection. Now, the USS Ronald Reagan is reporting positive COVID-19 cases and may have no option but to follow the lead of the Roosevelt. These events are warnings to our national security apparatus that pandemic diseases are clear and present threat to our Nation and her allies and interests. Koblentz and Hunzeker urge the US to recognize this threat and adjust to it with urgency and intensity. For more, Koblentz and Hunzeker’s article is available here.
 Summer Workshop on Pandemics, Bioterrorism, and Global Health Security
Summer Workshop on Pandemics, Bioterrorism, and Global Health Security
Are you registered for the summer workshop yet? From July 13-16, 2020, GMU Biodefense will be hosting a three and a half-day workshop on all things global health security. Leaders in the field will be discussing hot topics like COVID-19, pandemic preparedness, vaccine development, medical countermeasures, synthetic biology, and healthcare response to COVID-19. This is also a great networking opportunity as past participants come from a range of government agencies, NGOs, universities, think tanks, and foreign countries. Don’t miss out on the early-bird discount for this immersive workshop – you can register here.
Syria’s Chemical Weapons Attacks
The Organisation for the Prohibition of Chemical Weapons (OPCW) published its First Report by the Investigation and Identification Team, which strongly linked the Syrian government to the March 2017 sarin and chlorine attacks on a rebel town. Specifically, in March 2017, three projectiles – two containing sarin and one containing chlorine – were dropped from aircraft of the Syrian Arab Air Force into Ltamenah in northern Syria. In total, these weapons affected at least 106 individuals. The Washington Post reported on these findings and our own Dr. Gregory Koblentz, Director of the Biodefense Program, stated that strong evidence for attribution is the first concrete step toward punishing such violations of international laws and agreements. The OPCW is not a judicial body with the ability to determine and punish criminal acts, so action must be taken by the Executive Council and the Conference of the States Parties to the Chemical Weapons Convention, the United Nations Secretary-General, and the international community. The full report is available here.
 Smartphones and Contact Tracing
Smartphones and Contact Tracing
Contact tracing is a vital piece to not only public health response, but also helping “reopen” the country (keep reading for more insight into this). Unfortunately, it’s quite time and resource intensive and with widespread transmission and not enough public health resources, this can limit our capabilities. Some countries though, are looking to employe technology into contact tracing – “In Singapore, a country that’s turned to cellphone contact tracing, an app called TraceTogether uses Bluetooth to log when a user’s phone encounters another phone that has the app. If someone tests positive for COVID-19, he or she can easily submit a log of all the other people (and their phones) that he or she came in contact with in the last 21 days.” GMU’s HyunJung Kim has recently discussed this approach in South Korea – noting that “The disclosure of epidemic information is very significant for disease prevention and control, because we experienced the failure of disease control and prevention during the MERS of 2015,” HyunJung Kim, a PhD student in biodefense at George Mason University who has written about Korea’s public health system, says. “Information … makes people more comfortable because they can avoid and detour the areas/hospitals where infected people visited.” On the other hand though, such tech has ethical implications. Kelly Hills, Co-Principal of Rogue Bioethics noted that “We really have to keep our guard up against surveillance technologies that could be abused with very little effort, especially since these technologies are almost always going to be used against our most marginalized communities.” Damien P Williams, PhD candidate in the Department of Science, Technology, and Society at Virginia Tech recently noted that “First and foremost, supposedly anonymized tracking data sits alongside facial recognition as technologies which, in the current formulation of Western society, have no non-oppressive, non-exploitable use. Things developed and deployed in times of heightened fear and concern will very likely become every day violations.” Williams further stated that “Such a tool simply reinforces the trend toward surveillance technologies which are both insidiously abusive and also disproportionately leveraged against already-marginalized communities, as it has been the case with technologies and research in this vein, for literally centuries.” Where do you land on the topic?
Small Groups, Big Weapons: The Nexus of Emerging Tech and WMD Terrorism
A paradigm shift in recent years has seen non-state actors enhance their capabilities to utilize WMDs. A new report from the Combating Terrorism Center at West Point, is shedding light on the changes to capital, infrastructure, and intellectual capacity that are aiding this shift. “The commercialization of emerging technologies is reducing the financial, intellectual, and material barriers required for WMD development and employment. This report surveys three emerging technologies—synthetic biology, additive manufacturing (commonly known as 3D printing), and unmanned aerial systems—and examines the nexus of each with nuclear, biological, and chemical weapons agent proliferation. It examines how non-state actors might use these emerging technologies to overcome traditional barriers against the development and employment of WMD.” You can access the report here.
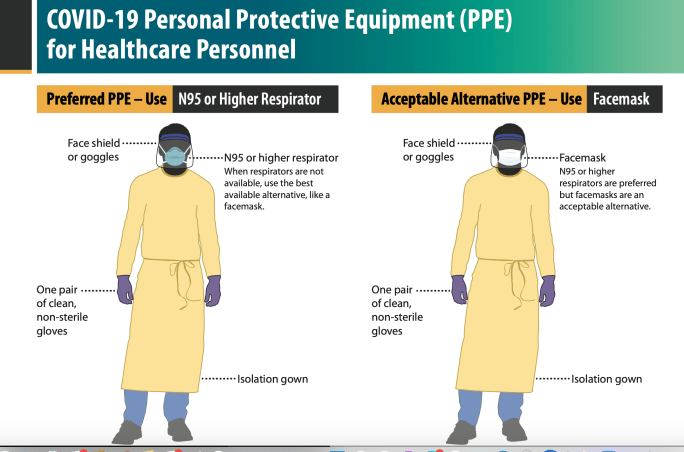
Inadequate PPE Distribution & Hospital Experiences Responding to COVID-19: A U.S. Survey
Just how well are hospitals managing the current pandemic? Not well. A survey by the HHS Office of the Inspector General (OIG) across U.S. hospitals from March 23-27, revealed some sobering insight into the challenges of COVID-19 response. 323 hospitals across 46 states chatted with the OIG on this (at least the hospital administrators did…). At a glance, the findings aren’t surprising – severe shortages of testing supplies, extended waits for results, widespread shortage of PPE, challenges maintaining adequate staffing and hospital capacity to treat patients, shortages of critical supplies and materials, and changing/sometimes inconsistent guidance. “Hospitals reported that changing and sometimes inconsistent guidance from Federal, State, and local authorities posed challenges and confused hospitals and the public. Hospitals reported that it was sometimes difficult to remain current with Centers for Disease Control and Prevention (CDC) guidance and that they received conflicting guidance from different government and medical authorities, including criteria for testing, determining which elective procedures to delay, use of PPE, and getting supplies from the national stockpile. Hospitals also reported concerns that public misinformation has increased hospital workloads (e.g., patients showing up unnecessarily, hospitals needing to do public education) at a critical time.” This is an insightful and telling report about the current challenges hospitals are facing in the U.S., not only in responding to COVID-19, but also preparing for it. Unfortunately, this isn’t the only report regarding inadequate supplies and distribution of PPE and vital medical supplies across the U.S. to various states. A new document has been released from HHS on the insufficient distribution of these critical pieces to healthcare response. “Only 11.7 million N95 respirator masks have been distributed nationwide—less than 1% of the 3.5 billion masks that the Trump Administration estimated would be necessary in the event of a severe pandemic. Only 7,920 ventilators have been distributed from the stockpile, even though a recent survey of 213 mayors—which did not include New York City, Chicago, or Seattle—identified a total estimated need of 139,000 ventilators.” Moreover, the report notes that the Strategic National Stockpile has made its last shipment of PPE for states as it now has 10% left, which will be reserved for federal workers and not distributed to states.
When Can We “Reopen” the U.S.?
The U.S. has over 427,000 cases and 14,696 deaths related to COVID-19, but many of us have been wondering, when will we be able to go back out to restaurants and congregate in public? The answer though, isn’t so simple and frankly, contingent upon a lot of factors like rapid testing and the ability to do contact tracing. First– “Number one: any given state that’s considering relaxing social distancing should have a demonstrated downward trend in cases over the two weeks prior. And we need to get better at being able to evaluate trend data across the country. Ultimately it would be good to have more data that would allow decision makers to be able to look at neighboring states and make sure they’re congruent with others in the region.” Beyond this and a sustained reduction in cases, we need widespread availability of PPE for healthcare workers. An adequately supplied healthcare infrastructure is critical and we must support healthcare workers as they face an onslaught of cases across the U.S.
Biodefense and Pandemic Policy
With each week, we learn more about ignored messages, red flags, and exercises that shed light on the very real failures in pandemic preparedness/response we are living right now. From the disbanding of the NSC global health security team to the failures in following the 69-page pandemic playbook, there have been several missteps and delays in the administration’s response. “The playbook was designed ‘so there wasn’t piecemeal thinking when trying to fight the next public health battle,’ said one former official who contributed to the playbook, warning that ‘the fog of war’ can lead to gaps in strategies.” Pandemic preparedness is no easy task, but many are looking at previous presidential responses to biological threats as an indicator that what we’re seeing now isn’t ideal. Within the most recent International Affairs journal, there is a reading list regarding global health crises that shed light on behavior norms and response measures during such events. In this collection, you’ll see GMU Biodefense professor and graduate program director Gregory Koblentz’s review of the Obama administration’s strategy for countering biology threats. “This strategy represents a shift in thinking away from the George W. Bush administration’s focus on biodefence, which emphasized preparing for and responding to biological weapon attacks, to the concept of biosecurity, which includes measures to prevent, prepare for and respond to naturally occurring and man-made biological threats.” The current COVID-19 pandemic will be a pivotal moment in biodefense and biosecurity policy, hopefully guiding future efforts and investments into pandemic preparedness.
 Student Spotlight: PREDICT-ing the Next Pandemic?
Student Spotlight: PREDICT-ing the Next Pandemic?
Michael Krug, a second-year student in the Biodefense MS program, November 2019 article highlights the critical need for comprehensive and quick biosurveillance tools to aid in pandemic preparedness. Last week, the decision was made to end USAID’s PREDICT project. PREDICT was established in 2009 to help develop wide-ranging detection capabilities; it was a component of the early-warning system. the project identified 1,200 viruses – including 160 novel coronaviruses – with the potential to induce a pandemic. Beyond identification, the project trained and supported staff across 60 foreign laboratories, such as the Wuhan Institute of Virology. Krug points out that the dissolution of PREDICT is an unfortunate reversal away from the US goal of slowing the emergence (or reemergence) of infectious diseases. This week, the LA Times reported on the termination of PREDICT, corroborating the echoed Krug’s sentiments and shared the announcement that the PREDICT program was just extended through September so that it can assist in the COVID-19 response.
Why Giving Americans Checks Makes Sense
In response to the March 22 column by Steven Pearlstein stating that providing funds to every American would be a bad idea, you can now read a rebuttal here. Included in this list of respondents is GMU Biodefense professor Sonia Ben Ouagrham-Gormley, who noted that “The plan to send money to every American may not be economically sound in normal circumstances, but it is an appropriate response to the economic hardships caused by this pandemic. And it could help curb the spread of the disease. True, many people will maintain their income, but what about the short-term burden people will face because of the pandemic? What about the employee who already lost her job and needs to care for her children? What about elderly people who have no one to rely on and who cannot stock up on food? These people need cash now to face the additional (temporary) economic burden caused by the epidemic. More important, they need it now to heed the Centers for Disease Control and Prevention’s guidelines: Stay home for a long enough period to break the transmission chain of the disease.”

 The U.S. Department of Health and Human Services has awarded
The U.S. Department of Health and Human Services has awarded