Happy Friday! We’re excited to give you some great updates on the world of global health security. Firstly, a recent cluster of what some are calling “rabies” has claimed the lives of 12 individuals. Officials are concerned as transmission seems to be spread through biting and the affected individuals do not appear to be experiencing pain or concern over decaying skin. Just kidding – April Fools’ Day! The zombie apocalypse hasn’t started (that I know of….), but the European Centre for Disease Prevention and Control (ECDC) has issued a warning about Yellow Fever in Angola. The ECDC is stressing the role of vaccination in travelers as a means to prevent the disease from traveling to susceptible populations. Researchers from the University of Sydney’s Charles Perkins Centre recently published their analysis regarding the barriers and facilitators for pathogens to jump species. They reviewed 203 human viruses to look at biological factors that may give us predictors as to which viruses are likely to emerge in human populations.
Mapping the Global Health Security Agenda
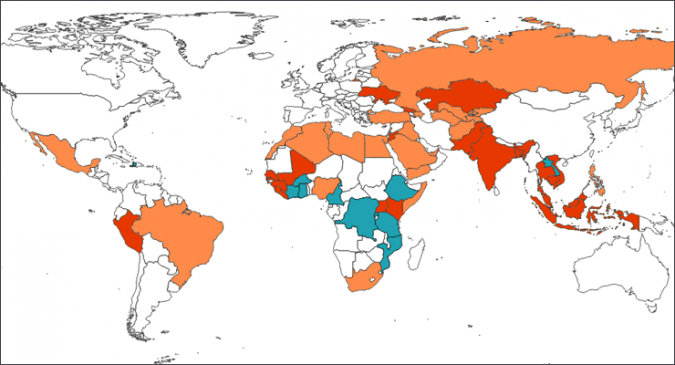
Raad Fadaak discusses the Global Health Security Agenda (GHSA) and its set of 11 Action Packages, working to better “prevent, detect, and respond to both human and animal infectious diseases threats.” Fighting an uphill war with organizational and political challenges, the GHSA has won some battles in the fight against global health security threats. In the midst of their MERS outbreak last year, South Korea looked to GHSA “to invest both diplomatic commitment as well as approximately $10 billion US dollars—in addition to graciously hosting the annual GHSA Ministerial High-Level Meeting.” Perhaps a challenging component to getting the GHSA and its Action Packages running smoothly is the vast array of partnerships and projects. Raad uses several wonderful spatial graphics to show timelines, participating countries, commitments, and much more in his analysis of GHSA. “Speaking more generally, it is important to not take the ‘global’ in ‘global health security’ for granted. These maps are a first step in helping to identify and isolate the unique scope and reach of US Governmental activity under GHSA programs – and the production of a specific kind of scalar policy through the GHSA.” In the midst of the Zika outbreak, now will be a telling time to see how the US will meet its commitments to the GHSA through the CDC and USAID.
Medical Rant & Response
Medical experiences tend to be low on the totem pole for “things I’d like to do with my day”. No one enjoys sitting in a busy emergency department waiting area, dealing with miscommunications, or waiting on lab results. Dallas, TX experienced first-hand the serious ramifications of medical frustrations when they had an Ebola patient stroll into their ED and then get discharged a few hours later. What happens when your symptoms are stumping physicians or the delivery of care is delayed? Researchers discuss an experience by a U.S. patient and “responses offered by several experts from various perspectives of the healthcare system.” As you read this article, consider your own healthcare experiences. Take it a step further and consider the global health security implications regarding some of these experiences…
How to (Make Chemical Weapons) Disappear Completely
GMU Biodefense MS student, Greg Mercer, is at it again! In this week’s commentary he’s discussing how chemical weapons are actually destroyed. Incineration and neutralization are the two most common practices employed by the US and Greg is breaking each technique down. Unfortunately, these methods aren’t aways perfect and can easily result in human and environmental damage. “Chemical weapons weren’t always disposed of so carefully, though. The James Martin Center for Nonproliferation Studies (CNS) cites at least 74 instances of the U.S. dumping chemical weapons at sea from 1918 to 1970.”
Ebola: We May have Won the Battle, But We Haven’t Won the War
It’s been two years since the first Ebola cases were identified in Guinea. Since then, you’ve surely read articles upon articles about the outbreak, how it spiraled out of control, and how we should’ve seen it coming. Why read more? History. Plain and simple – if we fail to study this outbreak and learn from all our mistakes, we’re doomed to repeat them. Ranging from infection and prevention control measures (music to my ears) to addressing the needs of Ebola survivors and social mobilization, there’s host of things we can learn. “And even when international partners responded, they often arrived too late. It took about three months from the time the United States announced in September 2014 it would send troops to Liberia to build Ebola treatment units (ETUs) to the time those were built. By then, the epidemic was already waning, and nine out of the eleven centers built never saw a patient.” What about fear? Fear became an issue not just on the ground in West Africa, but also in the U.S. after we started treating imported cases and the initial Dallas, TX case. “But I think we did most poorly when we let fear dictate the quality of the clinical care we provided to patients. ‘What if,’ Dr. Paul Farmer provokingly asked, ‘the fatality rate isn’t the virulence of the disease but the mediocrity of the medical delivery?’ Of course lack of staff, supplies and space, combined with an overwhelming patient load didn’t help.” Coordination, communication, and engagement. You may see these repeated several times whenever you read an after action report about this outbreak, and yet I’m not quite sure we’ve really let it sink in. Zika? Let’s just hope we can learn from the lessons of public health history before another outbreak sneaks up on us again. Update: two more cases have been identified in the now nine person cluster in Guinea. A young woman has died of Ebola in Liberia today, marking their first case in months.
 US knowledge gaps are the name of the game this week. 1/3 of Americans polled in a recent survey believed that Zika virus can be transmitted from coughing and sneezing. This same survey, conducted by a team from the Harvard T.H Chan School of Public Health and the National Public Health Information Coalition (NPHIC), found that people in households not affected by pregnancy issues held the most misconceptions about the virus. 39% thought that a non-pregnant woman’s illness could pose a threat to future birth defects. Brazil’s Health Ministry reported that the number of confirmed and suspected cases of microcephaly associated with Zika virus in the country have grown to 5,235 cases. The ministry also reported 19 infant deaths related to the virus. Revised estimates and a map released by the CDC now show that a larger percentage of the US population could be exposed to the virus as the mosquito season approaches . The University of Texas Medical Branch, Galveston (UTMB) has developed the first Zika animal model since the recent outbreak. “Several research institutions and companies have vaccine and drug candidates nearly ready to test, but until now a mouse model – a critical stage in preclinical testing – has not been available. The study, published this week in the American Journal of Tropical Medicine and Hygiene (AJTMH), removes a major bottleneck that was delaying treatment screening.” There is also concern regarding the ability for ultrasounds to fully detect brain damage and microcephaly in pregnant women with or exposed to Zika virus. If you’re looking to get your Zika on, attend the Zika Innovation Hack-a-thon April 2-3, 2016! As of March 30, 2016, there were 312 travel-associated Zika cases in the US.
US knowledge gaps are the name of the game this week. 1/3 of Americans polled in a recent survey believed that Zika virus can be transmitted from coughing and sneezing. This same survey, conducted by a team from the Harvard T.H Chan School of Public Health and the National Public Health Information Coalition (NPHIC), found that people in households not affected by pregnancy issues held the most misconceptions about the virus. 39% thought that a non-pregnant woman’s illness could pose a threat to future birth defects. Brazil’s Health Ministry reported that the number of confirmed and suspected cases of microcephaly associated with Zika virus in the country have grown to 5,235 cases. The ministry also reported 19 infant deaths related to the virus. Revised estimates and a map released by the CDC now show that a larger percentage of the US population could be exposed to the virus as the mosquito season approaches . The University of Texas Medical Branch, Galveston (UTMB) has developed the first Zika animal model since the recent outbreak. “Several research institutions and companies have vaccine and drug candidates nearly ready to test, but until now a mouse model – a critical stage in preclinical testing – has not been available. The study, published this week in the American Journal of Tropical Medicine and Hygiene (AJTMH), removes a major bottleneck that was delaying treatment screening.” There is also concern regarding the ability for ultrasounds to fully detect brain damage and microcephaly in pregnant women with or exposed to Zika virus. If you’re looking to get your Zika on, attend the Zika Innovation Hack-a-thon April 2-3, 2016! As of March 30, 2016, there were 312 travel-associated Zika cases in the US.
Stories You May Have Missed:
- Ancient Malaria Roots – researchers from Oregon State University are suggesting that the origins of malaria may have actually begun 100 million years ago. The protozoa genus, Plasmodium, has ancestral forms that may have used different insects during its evolution. “Scientists have argued and disagreed for a long time about how malaria evolved and how old it is,” Poinar said. “I think the fossil evidence shows that modern malaria vectored by mosquitoes is at least 20 million years old, and earlier forms of the disease, carried by biting midges, are at least 100 million years old and probably much older.”
- Ebola Is No Longer A Public Health Emergency of International Concern – On Tuesday, March 29th, 2016, the WHO Emergency Committee met, noting that since its last meeting, all three countries met criteria for interruption of original transmission chains. The WHO Direct General, Margaret Chan, stated that any trade and travel restrictions initiated during the outbreak should be lifted.
- Ethiopia Drought Emergency – Ethiopia is currently experiencing the worst drought it’s had in 50 years, causing water and food security issues. As of March 2016, over 10.2 million people need food assistance. Food security issues and poor access to water are severely impacting the agricultural industry as well as human health.
Enjoying your weekly dose of the Pandora Report? Sign up to receive it every week so the fun never ends!

One thought on “Pandora Report 4.1.2016”